

Operative mortality in colorectal cancer: prospective national study
- PMID: 14630754
- PMCID: PMC274053
- DOI: 10.1136/bmj.327.7425.1196
Operative mortality in colorectal cancer: prospective national study
Abstract
Objective: To develop a mathematical model that will predict the probability of death after surgery for colorectal cancer.
Design: Descriptive study using routinely collected clinical data.
Data source: The database of the Association of Coloproctology of Great Britain and Ireland (ACPGBI), encompassing 8077 patients with a new diagnosis of colorectal cancer in 73 hospitals during a 12 month period.
Statistical analysis: A three level hierarchical logistic regression model was used to identify independent predictors of operative mortality. The model was developed on 60% of the patient population and its validity tested on the remaining 40%.
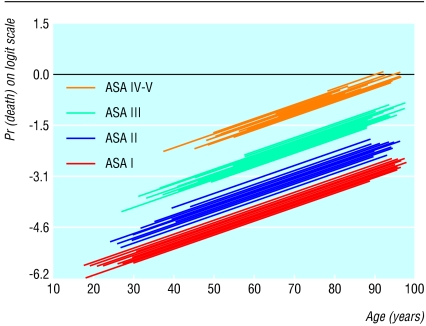
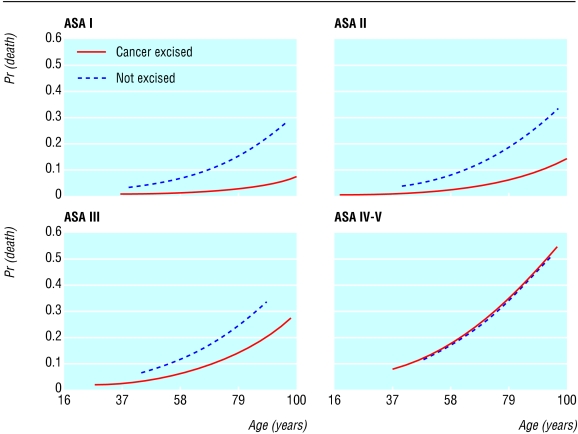
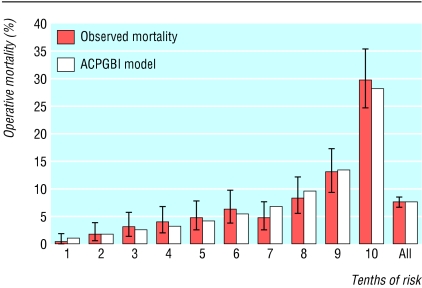
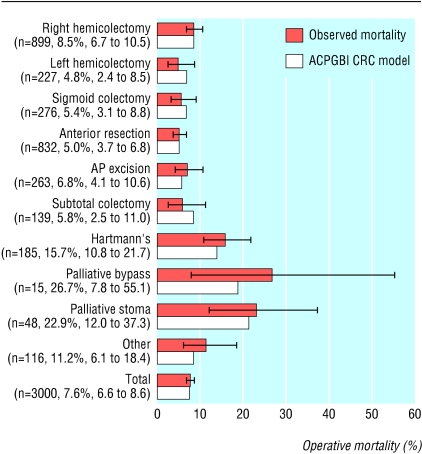
Results: Overall postoperative mortality was 7.5% (95% confidence interval 6.9% to 8.1%). Independent predictors of death were age, American Society of Anesthesiology (ASA) grade, Dukes's stage, urgency of the operation, and cancer excision. When tested the predictive model showed good discrimination (area under the receiver operating characteristic curve = (0.775) and calibration (comparison of observed with expected mortality across different procedures; Hosmer-Lemeshow statistic = 6.34, 8 df, P = 0.610).
Conclusions: Clinicians can predict postoperative death by using a simple numerical table derived from the statistical model of the ACPGBI. The model can be used in everyday practice for preoperative counselling of patients and their carers as a part of multidisciplinary care. It may also be used to compare the outcomes between multidisciplinary teams for colorectal cancer.
Figures
References
-
- Spiegelhalter DJ, Aylin P, Best NG, Evans SJW, Murray GD. Commissioned analysis of surgical performance by using routine data: lessons from Bristol inquiry. J R Statist Soc A 2002;165: 1-31.
-
- The Association of Coloproctology of Great Britain and Ireland Database and Dataset [computer program]. Version 2 for Access 2000. (UK):ClinIT 2000. www.cancernw.org.uk/clinit/products.htm?productindex = 1 (accessed 23 Mar 2003).
-
- Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA 1963;178: 261-6. - PubMed
-
- Department of Health. Hospital episode statistics, Main operations 2000/01. www.doh.gov.uk/hes/standard_data/available_tables/main_operations/index..... (accessed 23 Mar 2003).
-
- Callum KG, Gray AJG, Hoile RN, Ingram GS, Martin IC, Sherry KM, et al. Appendix A. In: Then and now: the 2000 report of the national confidential enquiry into perioperative deaths. London: NCEPOD, 2000: 125-6.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous