

Microvascular reconstructions of full-thickness oncological chest wall defects
- PMID: 14631216
- PMCID: PMC1356161
- DOI: 10.1097/01.sla.0000098626.79986.51
Microvascular reconstructions of full-thickness oncological chest wall defects
Abstract
Objective: To evaluate the suitability of microvascular flaps for the reconstruction of extensive full-thickness defects of the chest wall.
Summary background data: Chest wall defects are conventionally reconstructed with pedicular musculocutaneous flaps or the omentum. Sometimes, however, these flaps have already been used, are not reliable due to previous operations or radiotherapy, or are of inadequate size. In such cases, microvascular flaps offer the only option for reconstruction.
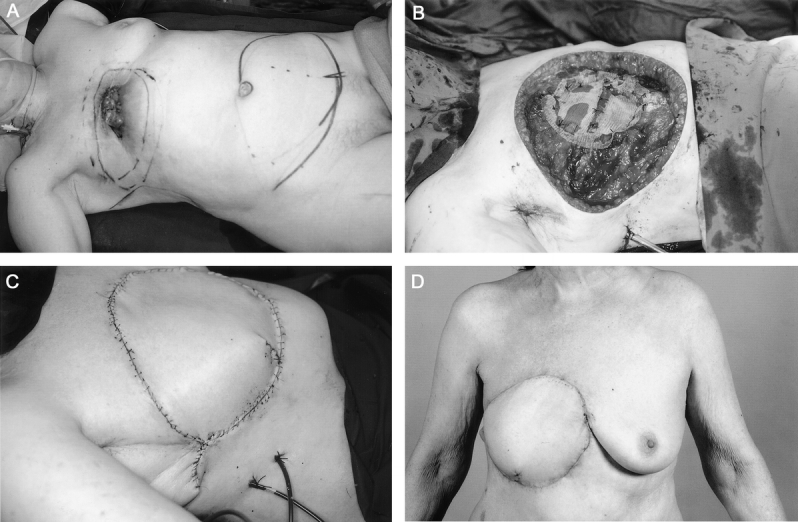
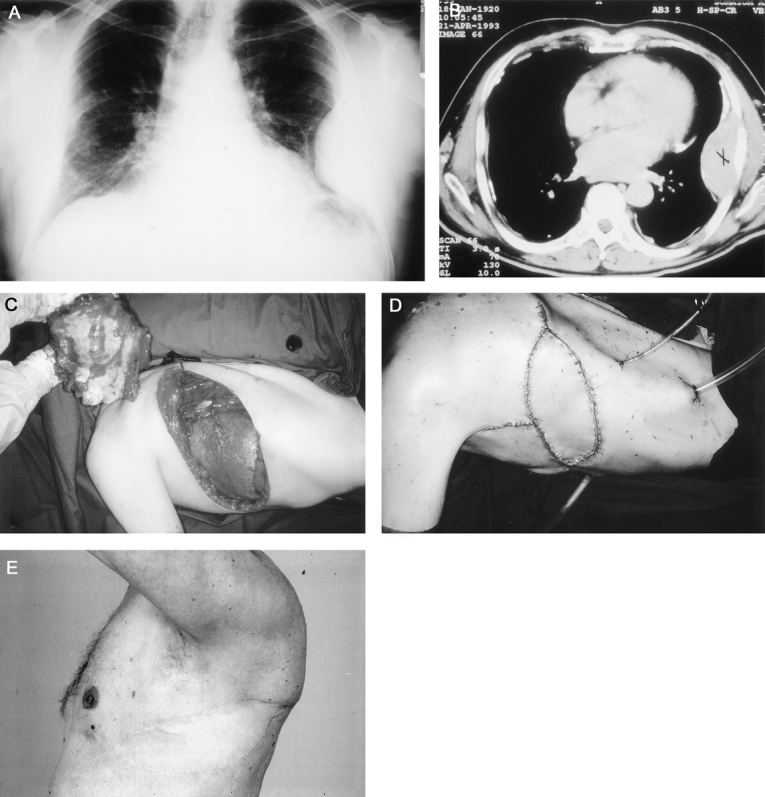
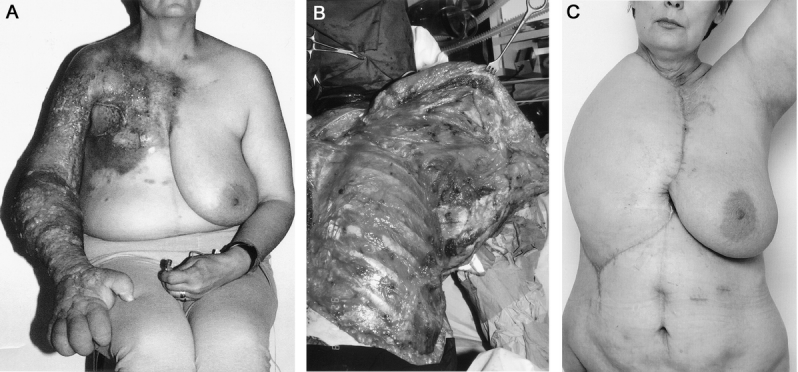
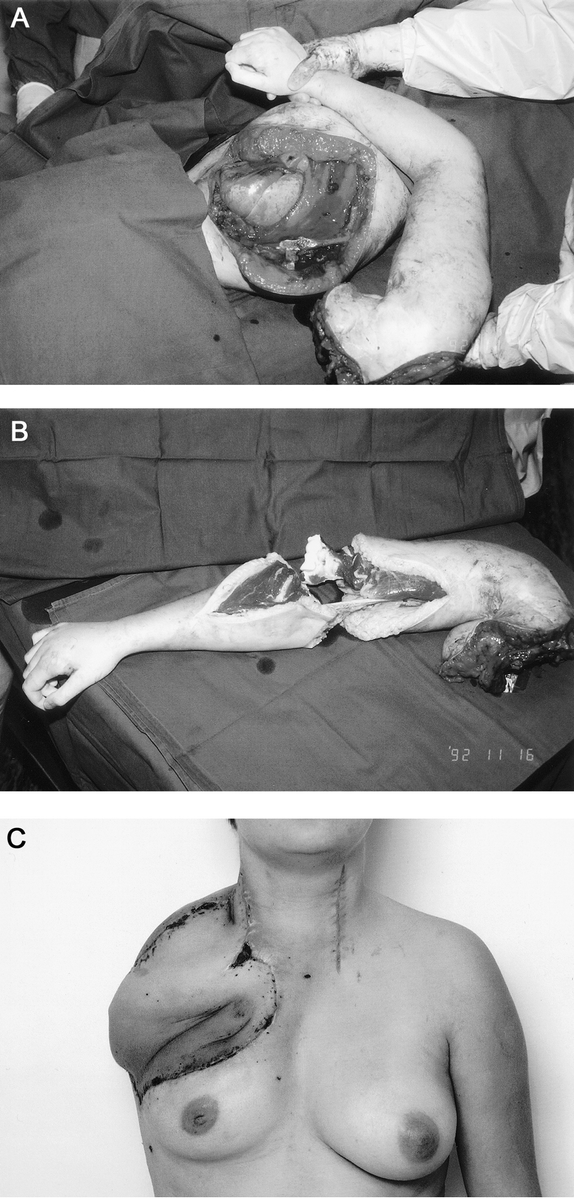
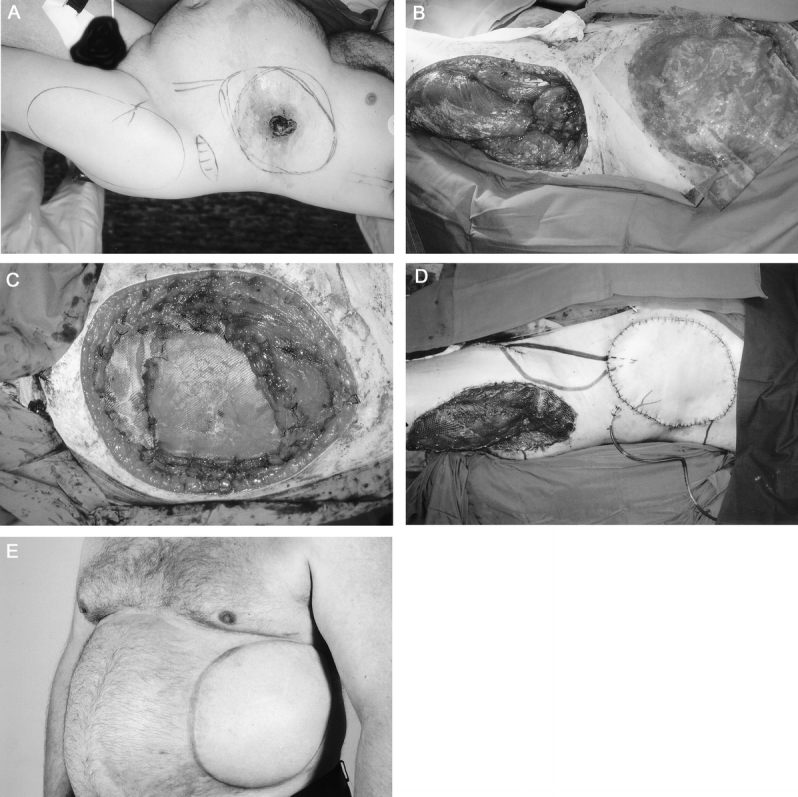
Methods: From 1988 to 2001, 26 patients with full-thickness resections of the chest wall underwent reconstruction with microvascular flaps. There were 8 soft tissue sarcomas, 8 recurrent breast cancers, 5 chondrosarcomas, 2 desmoid tumors, 1 large cell pulmonary cancer metastasis, 1 renal cancer metastasis, and 1 bronchopleural fistula. The surgery comprised 5 extended forequarter amputations, 5 lateral resections, 8 thoracoabdominal resections, and 8 sternal resections. The mean diameter of a resection was 28 cm. The soft tissue defect was reconstructed with 16 tensor fasciae latae, 5 tensor fascia latae combined with rectus femoris, and 3 transversus rectus abdominis myocutaneous flaps. In 2 patients with a forequarter amputation, the remnant forearm was used as the osteomusculocutaneous free flap.
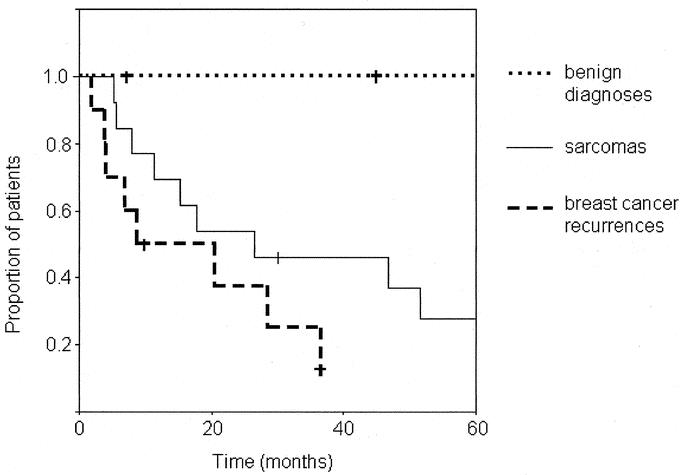
Results: There were no flap losses or perioperative mortality. Four patients needed tracheostomy owing to prolonged respiratory difficulties. The mean survival time for patients with sarcomas was 39 months and for those with recurrent breast cancer 18 months.
Conclusions: Extensive chest wall resections are possible with acceptable results. In patients with breast cancer, the surgery may offer valuable palliation and in those with sarcomas it can be curative.
Figures
Comment in
-
Microvascular reconstructions of full-thickness oncological chest wall defects.Ann Surg. 2004 Sep;240(3):558-9; author reply 559. doi: 10.1097/01.sla.0000138823.11342.25. Ann Surg. 2004. PMID: 15319729 Free PMC article. No abstract available.
References
-
- Incarbone M, Pastorino U. Surgical treatment of chest wall tumors. World J Surg. 2001;25:218–230. - PubMed
-
- Vandeweyer E, Nogaret JM, Hertens D, et al. Chest coverage and reconstruction after recurrence of breast cancer. Eur J Plast Surg. 2002;25:7–10.
-
- Chapelier AR, Bacha EA, de Montpreville VT, et al. Radical resection of radiation-induced sarcoma of the chest wall: report of 15 cases. Ann Thorac Surg. 1997;63:214–219. - PubMed
-
- Cordeiro PG, Santamaria E, Hidalgo D. The role of microsurgery in reconstruction of oncologic chest wall defects. Plast Reconstr Surg. 2001;108:1924–1930. - PubMed
-
- Arnold PG, Pairolero PC. Chest-wall reconstruction: an account of 500 consecutive patients. Plast Reconstr Surg. 1996;98:804–810. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
