

Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis
- PMID: 14631217
- PMCID: PMC1356162
- DOI: 10.1097/01.sla.0000098624.04100.b1
Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis
Abstract
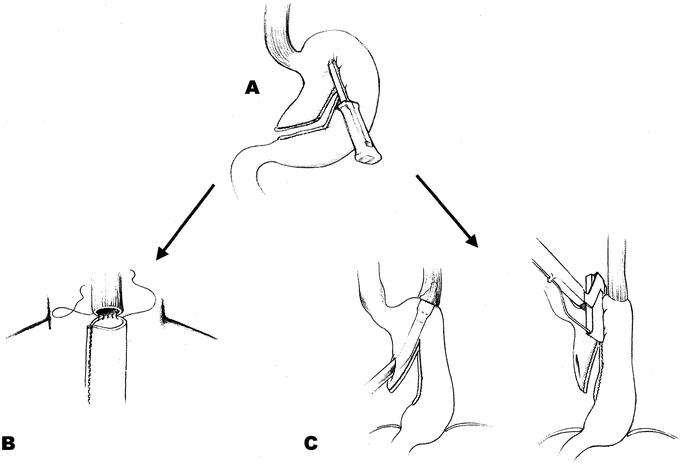
Objective: The purpose of the study was to compare in prospective randomized fashion a manually sutured esophagogastric anastomosis in the neck and a stapled in the chest after esophageal resection and gastric tube reconstruction.
Summary background data: Despite the fact that all reconstructions after esophagectomy will result in a cervical or a thoracic anastomosis, controversy still exists as to the optimal site for the anastomosis. In uncontrolled studies, both neck and chest anastomoses have been advocated. The only reported randomized study is difficult to evaluate because of varying routes of the substitute and different anastomotic techniques within the groups. The reported high failure rate of stapled anastomoses in the neck and the fact that most surgeons prefer to suture cervical anastomoses made us choose this technique for anastomosis in the neck. Our routine and the preference of most surgeons to staple high thoracic anastomoses became decisive for type of thoracic anastomoses.
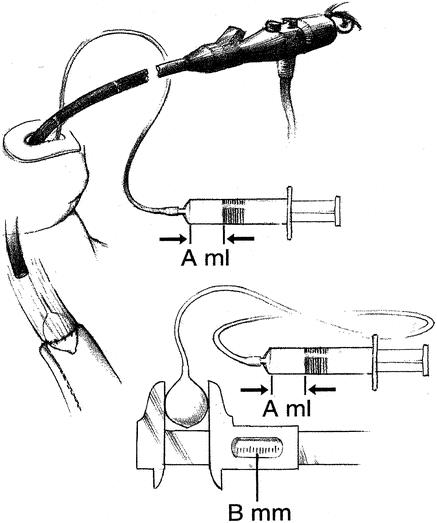
Methods: Between May 9, 1990 and February 5, 1996, 83 patients undergoing esophageal resection were prospectively randomized to receive an esophagogastric anastomosis in the neck (41 patients) or an esophagogastric anastomosis in the chest (42 patients). To evaluate selection bias, patients undergoing esophageal resection during the same period but not randomized (n = 29) were also followed and compared with those in the study (n = 83). Objective measurements of anastomotic level and diameter were assessed with an endoscope and balloon catheter 3, 6, and 12 months after surgery. The long-term survival rates were compared with the log-rank test.
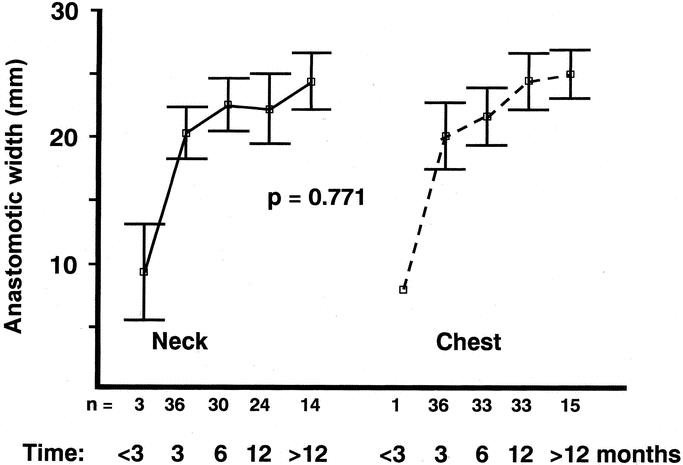
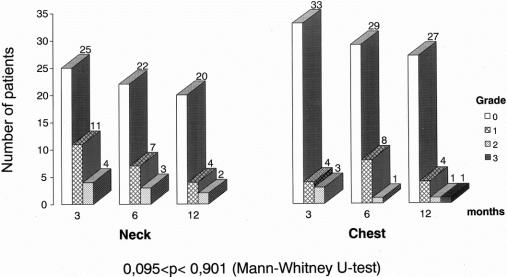
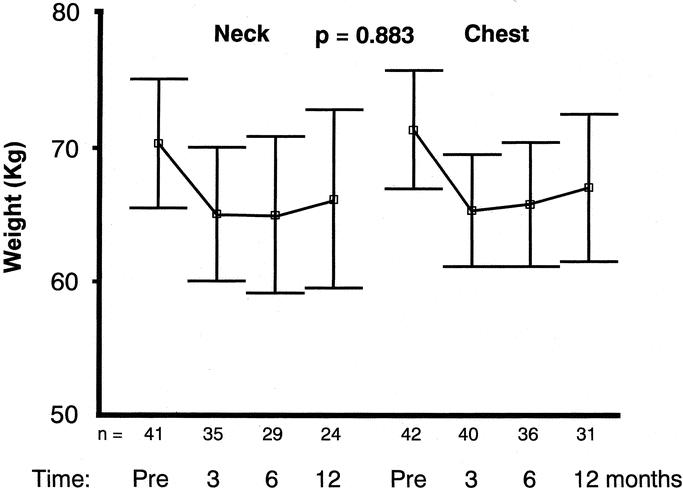
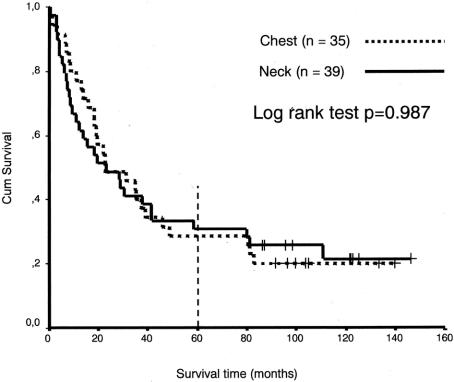
Results: Two patients (1.8%) died in hospital, and the remaining 110 patients were followed until death or for a minimum of 60 months. The genuine 5-year survival rate was 29% for chest anastomoses and 30% for neck anastomoses. The overall leakage rate was 1.8% (2 cases of 112) with no relation to mortality or anastomotic method. All patients in the randomized group had tumor-free proximal and distal resection lines, but 1 patient in the nonrandomized group had tumor infiltrates in the proximal resection margin. At 3, 6, and 12 months after operation, there was no difference in anastomotic diameter between the esophagogastric anastomosis in the neck and in the thorax (P = 0.771), and both increased with time (P = 0.004, ANOVA repeated measures). Body weight development was the same in the two groups. With similar results in randomized and nonrandomized patients, study bias was eliminated.
Conclusions: When performed in a standardized way, neck and chest anastomoses after esophageal resection are equally safe. The additional esophageal resection of 5 cm in the neck group did not increase tumor removal and survival; on the other hand, it did not adversely influence morbidity, anastomotic diameter, or eating as reflected by body weight development.
Figures
Comment in
-
Esophageal cancer: is there hope?Curr Surg. 2005 Mar-Apr;62(2):150-5; quiz 155. doi: 10.1016/j.cursur.2004.09.006. Curr Surg. 2005. PMID: 15796933 No abstract available.
References
-
- Urschel JD. Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surg. 1995;169:634–640. - PubMed
-
- Müller JM, Erasmi H, Stelzner M, et al. Surgical therapy of oesophageal carcinoma. Br J Surg. 1990;77:845–857. - PubMed
-
- Lam TCF, Fok M, Cheng SWK, et al. Anastomotic complications after esophagectomy for cancer: a comparison of neck and chest anastomoses. J Thorac Cardiovasc Surg. 1992;104:395–400. - PubMed
-
- Patil PK, Patel SG, Mistry RC, et al. Cancer of the esophagus: esophagogastric anastomotic leak - a retrospective study of predisposing factors. J Surg Oncol. 1992;49:163–167. - PubMed
-
- Chasseray VM, Kiroff GK, Buard JL, et al. Cervical or thoracic anastomosis for esophagectomy for carcinoma. Surg Gynecol Obstet. 1989;169:55–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
