

Right living donor liver transplantation: an option for adult patients: single institution experience with 74 patients
- PMID: 14631222
- PMCID: PMC1356167
- DOI: 10.1097/01.sla.0000098619.71694.74
Right living donor liver transplantation: an option for adult patients: single institution experience with 74 patients
Abstract
Objective: To present an institutional experience with the use of right liver grafts in adult patients and to assess the practicability and efficacy of this procedure by analyzing the results.
Summary background data: Living donor liver transplantation (LDLT) for the pediatric population has gained worldwide acceptance. In the past few years, LDLT has also become feasible for adult patients due to technical evolution in hepatobiliary surgery and increased experience with reduced-size and split-liver transplants. Nevertheless, some graft losses remain unexplained and are possibly due to unrecognized venous outflow problems.
Methods: From April 1998 to September 2002, we performed 74 right LDLTs (segments 5-8). The 74 donors were selected from 474 candidates according to standard protocol. The median age of the donors was 35 years (range 18-58 years) and 51 years (range 18-64 years) in recipients. Standard and extended indications for transplantation were considered. Over the period reported, technical modifications in the bile duct anastomosis (duct-to-duct, end-to-end, or end-to-side) and a new graft implantation technique that provides maximized venous outflow, leading to outcome improvement, were developed.
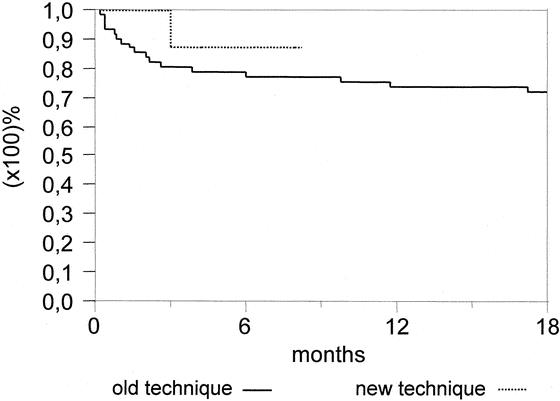
Results: 64.9% of patients had liver cirrhosis and 35.1% had malignancy. While 44 donors (59.5%) presented an uneventful postoperative course, 27% minor (pleural effusion, pneumonia, venous thrombosis, wound infection, incisional hernia) and 13.5% major (biliary leakage, death of a donor due to unrecognized hereditary liver disease, and consecutive liver insufficiency) complications were documented. In recipients, 23% biliary complications and 6.8% hepatic artery thrombosis occurred. The overall patient and graft survival rate after 1 year was 79.4% and 75.3%, respectively. In cases with extended indication, the patient survival rate was 74% and the graft survival rate 68% at 12 months. Using technical modifications in the last 10 recipients, including 2 critically decompensated cirrhotics, the survival rate was 100% at a median follow-up of 3.5 months.
Conclusions: In our transplant program, living donor liver transplantation has become a standard option in the adult patient population. The critical issue of this procedure is donor morbidity. Technical improvements in the harvesting and implantation of right grafts can also offer hope to patients with challenging forms of end-stage liver disease or malignant liver tumors.
Figures





References
-
- Eurotransplant International Foundation. Available at: http://www.eurotransplant.nl/. Accessed January 30, 2003.
-
- Kam I. Adult-adult right hepatic lobe living donor liver transplantation for status 2a patients: too little, too late [editorial]. Liver Transpl. 2002;8:347-349. - PubMed
-
- Beavers KL, Sandler RS, Fair JH, et al. The living donor experience: donor health assessment and outcomes after living donor liver transplantation. Liver Transpl. 2001;7:943-947. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
