

Liver resection for colorectal metastases: the third hepatectomy
- PMID: 14631224
- PMCID: PMC1356169
- DOI: 10.1097/01.sla.0000098112.04758.4e
Liver resection for colorectal metastases: the third hepatectomy
Abstract
Objective: To determine the risk, the benefit, and the main factors of prognosis of third liver resections for recurrent colorectal metastases.
Summary background data: Recurrence following liver resection is frequent after a first as after a second hepatectomy. Second liver resections yield a similar survival to that obtained with first liver resection, but little is known about third hepatectomy.
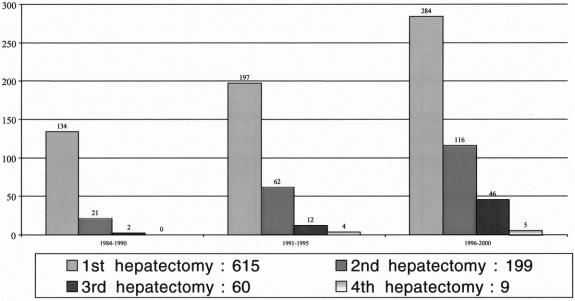
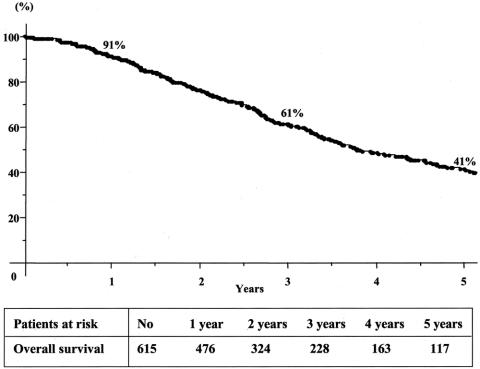
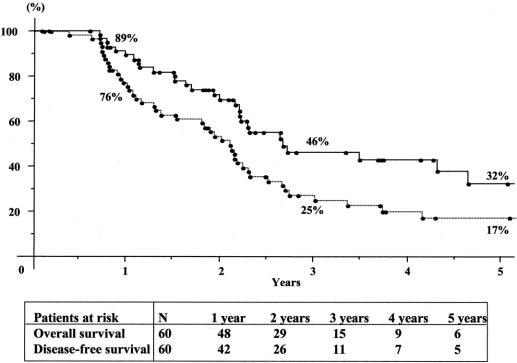
Methods: This study reports a retrospective analysis of 60 patients who underwent a third liver resection for colorectal metastases in a 16-year experience (1984-2000). Patients were identified from a prospective database that collected 615 consecutive patients who cumulated 883 hepatectomies (615 first, 199 second, 60 thirds, and 9 fourths). Third hepatic resections were compared with first and second procedures, in terms of risk and benefit for the patient. Prognostic factors of survival after third hepatic resection were determined by univariate and multivariate analysis.
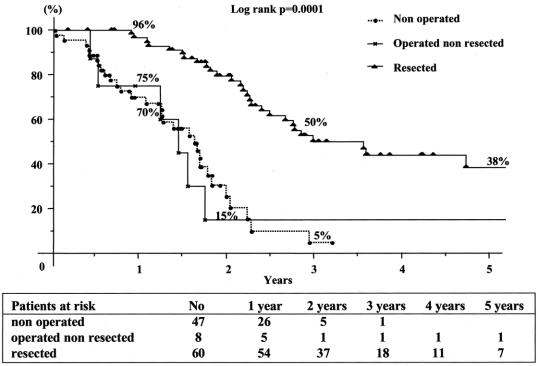
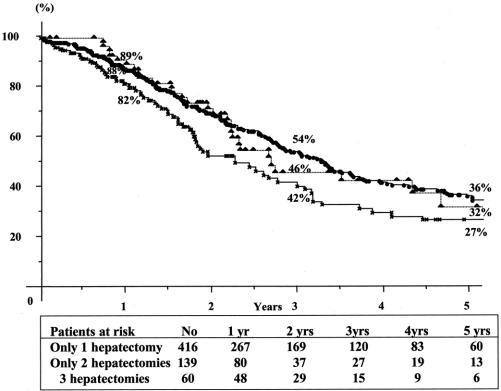
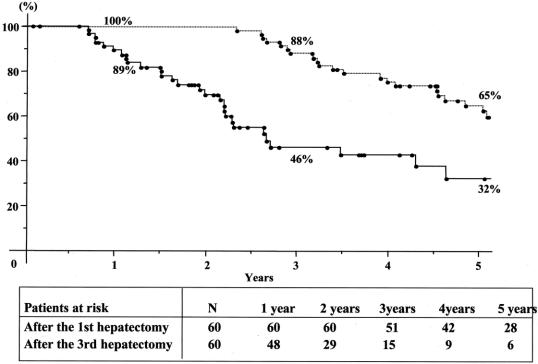
Results: A third hepatic resection was attempted in 68 of 115 of liver recurrences following a second hepatectomy (59%) and achieved in 88% of the cases (60 of 68). There was no intraoperative mortality or postoperative deaths within the 2 months. Fifteen patients developed postoperative complications (25%), a rate similar to that of first and second hepatectomies. Overall 5-year survival was 32% and disease-free survival was 17% after the third resection. Survival compared favorably to that of patients with recurrence following a second hepatectomy who could not be operated (5% at 3 years) or who failed to be resected (15% at 2 years, P = 0.0001). It also compared favorably to that of patients who underwent only two hepatectomies (5-year survival, 27%). When estimated from the time of first hepatectomy, survival was 65% at 5 years for the 60 patients who underwent three hepatic resections. Concomitant extrahepatic tumor was treated in 16 patients (27%) by 11 abdominal procedures and 5 pulmonary resections. By multivariate analysis, tumor size > 30 mm for first liver metastases, presence of extrahepatic tumor at second hepatectomy, and noncurative pattern of third liver resection were independent prognostic factors of reduced survival.
Conclusions: Third hepatectomy is safe and provides an additional benefit of survival similar to that of first and second liver resections. It is worthwhile when curative and integrated into an intended multimodal strategy of tumoral eradication.
Figures
References
-
- Hughes KS, Simon R, Songhorabodi S, et al. Resection of the liver for colorectal carcinoma metastases: a multi-institutional study of patterns of recurrence. Surgery. 1986;100:278–284. - PubMed
-
- Scheele J, Stangl R, Altendorf-Hofmann A, et al. Indicators of prognosis after hepatic resection for colorectal secondaries. Surgery. 1991;110:13–29. - PubMed
-
- Nordlinger B, Jaeck D, Guiguet M, et al. Surgical resection of hepatic metastases: multicentric retrospective study by the French Association of Surgery. In: Nordlinger B, Jaeck D, eds. Treatment of Hepatic Metastases of Colorectal Cancer. New York: Springer-Verlag, 1992:129–146.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
