

Anorectal melanoma: surgical management guidelines according to tumour thickness
- PMID: 14647131
- PMCID: PMC2376860
- DOI: 10.1038/sj.bjc.6601409
Anorectal melanoma: surgical management guidelines according to tumour thickness
Abstract
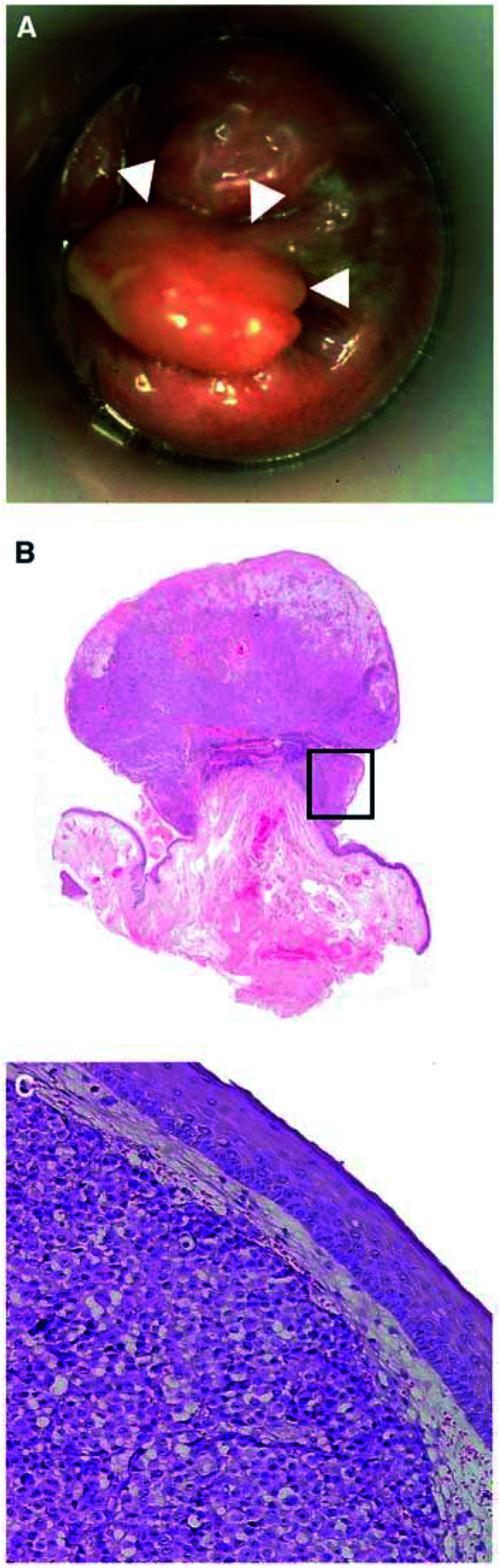
Management of patients with anorectal melanoma is still controversial. To reach a rationale therapeutic approach, we reviewed our experience obtained over the past decade. In all, 19 consecutive patients with the diagnosis of anorectal melanoma were included in this retrospective survey. Details of the patients' presentation, symptoms, tumour size and histology and tumour state were recorded, and the primary therapeutic procedures were evaluated in detail. The size of the tumours ranged between 0.5 and 7 cm in diameter. The median tumour thickness was 10 mm (range 0.6-40 mm). At diagnosis, six of 19 patients already presented with either regional or distant metastases. The remaining 13 patients were treated with curative intend, either by abdomino-perineal resection (APR) or wide local excision (WLE). The form of operative therapy, however, had no impact on overall survival. Nevertheless, the incidence of local recurrences was lower after APR even for patients with less favourable tumours. In conclusion, WLE alone is not sufficient for local tumour control of thick anorectal melanoma.
Figures
References
-
- Abbas JS, Karakousis CP, Holyoke D (1980) Ano-rectal melanoma: clinical features, recurrence and patient survival. Int Surg 65: 423–426 - PubMed
-
- Ballo MT, Gershenwald JE, Zagars GK, Lee JE, Mansfield PF (2002) Sphincter–sparing local excision and ádjuvant radiation for anal–rectal melanoma. J Clin Onc0l 20(23): 4555–4558 - PubMed
-
- Brady MS, Kavolius JP, Quan SHQ (1995) Anorectal melanoma a 64-years experience at memorial Sloan-Kettering Cancer Center. Dis Colon Rectum 38(2): 146–151 - PubMed
-
- Chung AF, Casey MJ, Flannery JT, Woodruff JM, Lewis JL (1980) Malignant melanoma of the vagina: a report of 19 cases. Obstet Gynecol 55: 720–727 - PubMed
-
- Going JJ, Kean DM (1989) Malignant melanoma of the nasal cavity. J Laryngol Otol 103: 231–233 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
