

Magnetic resonance fluoroscopy allows targeted delivery of mesenchymal stem cells to infarct borders in Swine
- PMID: 14656911
- PMCID: PMC1325104
- DOI: 10.1161/01.CIR.0000095790.28368.F9
Magnetic resonance fluoroscopy allows targeted delivery of mesenchymal stem cells to infarct borders in Swine
Abstract
Background: The local environment of delivered mesenchymal stem cells (MSCs) may affect their ultimate phenotype. MR fluoroscopy has the potential to guide intramyocardial MSC injection to desirable targets, such as the border between infarcted and normal tissue. We tested the ability to (1) identify infarcts, (2) navigate injection catheters to preselected targets, (3) inject safely even into fresh infarcts, and (4) confirm injection success immediately.
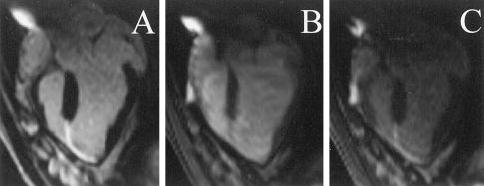
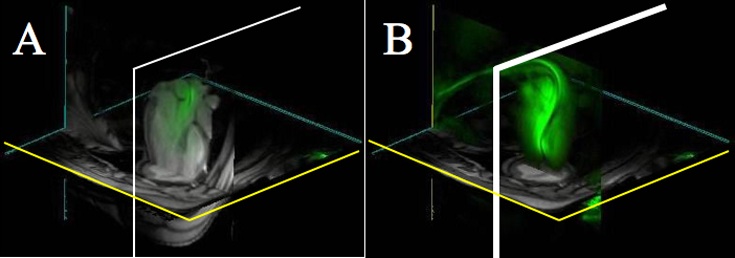
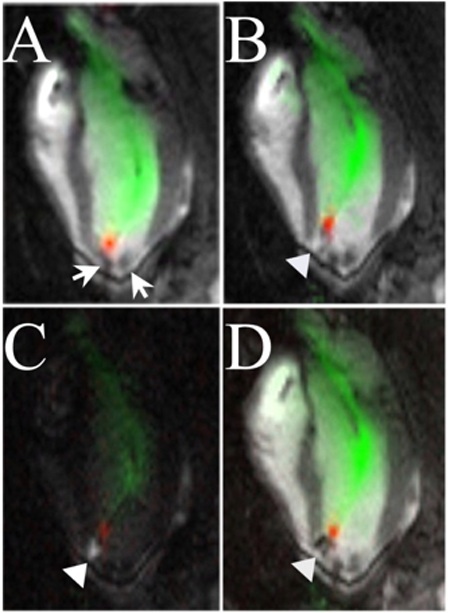
Methods and results: A 1.5-T MRI scanner was customized for interventional use, with rapid imaging, independent color highlighting of catheter channels, multiple-slice 3D rendering, catheter-only viewing mode, and infarct-enhanced imaging. MRI receiver coils were incorporated into guiding catheters and injection needles. These devices were tested for heating and used for targeted MSC delivery. In infarcted pigs, myocardium was targeted by MR fluoroscopy. Infarct-enhanced imaging included both saturation preparation MRI after intravenous gadolinium and wall motion. Porcine MSCs were MRI-labeled with iron-fluorescent particles. Catheter navigation and multiple cell injections were performed entirely with MR fluoroscopy at 8 frames/s with 1.7x3.3x8-mm voxels. Infarct-enhanced MR fluoroscopy permitted excellent delineation of infarct borders. All injections were safely and successfully delivered to their preselected targets, including infarct borders. Iron-fluorescent particle-labeled MSCs were readily visible on delivery in vivo and post mortem.
Conclusions: Precise targeted delivery of potentially regenerative cellular treatments to recent myocardial infarction borders is feasible with an MR catheter delivery system. MR fluoroscopy permits visualization of catheter navigation, myocardial function, infarct borders, and labeled cells after injection.
Figures


References
-
- Wang JS, Shum-Tim D, Chedrawy E, et al. The coronary delivery of marrow stromal cells for myocardial regeneration: pathophysiologic and therapeutic implications. J Thorac Cardiovasc Surg. 2001;122:699–705. - PubMed
-
- Orlic D, Kajstura J, Chimenti S, et al. Bone marrow cells regenerate infarcted myocardium. Nature. 2001;410:701–705. - PubMed
-
- Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potential of adult human mesenchymal stem cells. Science. 1999;284:143–147. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
