

Comparison of sequential three-drug regimens as initial therapy for HIV-1 infection
- PMID: 14668455
- PMCID: PMC4767257
- DOI: 10.1056/NEJMoa030264
Comparison of sequential three-drug regimens as initial therapy for HIV-1 infection
Abstract
Background: The optimal sequencing of antiretroviral regimens for the treatment of infection with human immunodeficiency virus type 1 (HIV-1) is unknown. We compared several different antiretroviral treatment strategies.
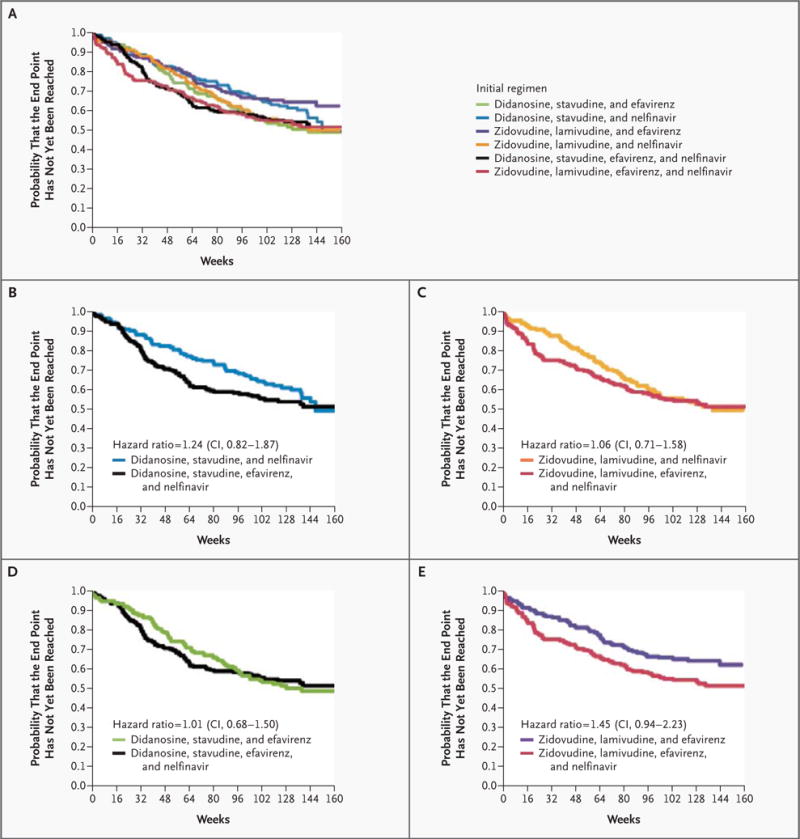
Methods: This multicenter, randomized, partially double-blind trial used a factorial design to compare pairs of sequential three-drug regimens, starting with a regimen including zidovudine and lamivudine or a regimen including didanosine and stavudine in combination with either nelfinavir or efavirenz. The primary end point was the length of time to the failure of the second three-drug regimen.
Results: A total of 620 subjects who had not previously received antiretroviral therapy were followed for a median of 2.3 years. Starting with a three-drug regimen containing efavirenz combined with zidovudine and lamivudine (but not efavirenz combined with didanosine and stavudine) appeared to delay the failure of the second regimen, as compared with starting with a regimen containing nelfinavir (hazard ratio for failure of the second regimen, 0.71; 95 percent confidence interval, 0.48 to 1.06), as well as to delay the second virologic failure (hazard ratio, 0.56; 95 percent confidence interval, 0.29 to 1.09), and significantly delayed the failure of the first regimen (hazard ratio, 0.39) and the first virologic failure (hazard ratio, 0.34). Starting with zidovudine and lamivudine combined with efavirenz (but not zidovudine and lamivudine combined with nelfinavir) appeared to delay the failure of the second regimen, as compared with starting with didanosine and stavudine (hazard ratio, 0.68), and significantly delayed both the first and the second virologic failures (hazard ratio for the first virologic failure, 0.39; hazard ratio for the second virologic failure, 0.47), as well as the failure of the first regimen (hazard ratio, 0.35). The initial use of zidovudine, lamivudine, and efavirenz resulted in a shorter time to viral suppression.
Conclusions: The efficacy of antiretroviral drugs depends on how they are combined. The combination of zidovudine, lamivudine, and efavirenz is superior to the other antiretroviral regimens used as initial therapy in this study.
Copyright 2003 Massachusetts Medical Society
Figures



Comment in
-
HIV therapy--what do we know, and when do we know it?N Engl J Med. 2003 Dec 11;349(24):2351-2. doi: 10.1056/NEJMe038173. N Engl J Med. 2003. PMID: 14668462 No abstract available.
-
Comparison of regimens as initial therapy for HIV.N Engl J Med. 2004 Mar 4;350(10):1053-4; author reply 1053-4. doi: 10.1056/NEJM200403043501018. N Engl J Med. 2004. PMID: 14999120 No abstract available.
References
-
- Paredes R, Mocroft A, Kirk O, et al. Predictors of virological success and ensuing failure in HIV-positive patients starting highly active antiretroviral therapy in Europe: results from the EuroSIDA study. Arch Intern Med. 2000;160:1123–32. - PubMed
-
- Ledergerber B, Egger M, Opravil M, et al. Clinical progression and virological failure on highly active antiretroviral therapy in HIV-1 patients: a prospective cohort study. Lancet. 1999;353:863–8. - PubMed
-
- Grabar S, Pradier C, Le Corfec E, et al. Factors associated with clinical and virological failure in patients receiving a triple therapy including a protease inhibitor. AIDS. 2000;14:141–9. - PubMed
-
- Department of Health and Human Services Panel on Clinical Practices for Treatment of HIV Infection. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. (Accessed November 12, 2003, at http://www.aidsinfo.nih.gov/guidelines/adult/archive/AA_071403.html.) - PubMed
-
- Yeni PG, Hammer SM, Carpenter CC, et al. Antiretroviral treatment for adult HIV infection in 2002: updated recommendations of the International AIDS Society–USA Panel. JAMA. 2002;288:222–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RR00070/RR/NCRR NIH HHS/United States
- AI38858/AI/NIAID NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- RR05096/RR/NCRR NIH HHS/United States
- M01 RR005096/RR/NCRR NIH HHS/United States
- RR00044/RR/NCRR NIH HHS/United States
- M01 RR000044/RR/NCRR NIH HHS/United States
- R01 AI046148/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- RR00052/RR/NCRR NIH HHS/United States
- AI38855/AI/NIAID NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical