

Balloon aortic valvoplasty in paediatric patients: progressive aortic regurgitation is common
- PMID: 14676250
- PMCID: PMC1768038
- DOI: 10.1136/heart.90.1.77
Balloon aortic valvoplasty in paediatric patients: progressive aortic regurgitation is common
Abstract
Objective: To evaluate immediate and midterm results after balloon valvoplasty in a paediatric population with congenital aortic stenosis, giving special consideration to aortic regurgitation.
Design: Retrospective study.
Setting: Two tertiary referral centres for paediatric cardiology.
Patients: 70 consecutive patients, with an age range of 0-16.4 years. Group A infants < 3 months old (n = 21). Group B children > 3 months old (n = 49). Median follow up time was 19.8 months, range 0-158 months.
Intervention: All patients underwent balloon aortic valvoplasty. The balloon to annulus ratio was selected at a mean of 0.90 (range 0.67-1.0).
Main outcome measures: Doppler gradients and degree of aortic regurgitation.
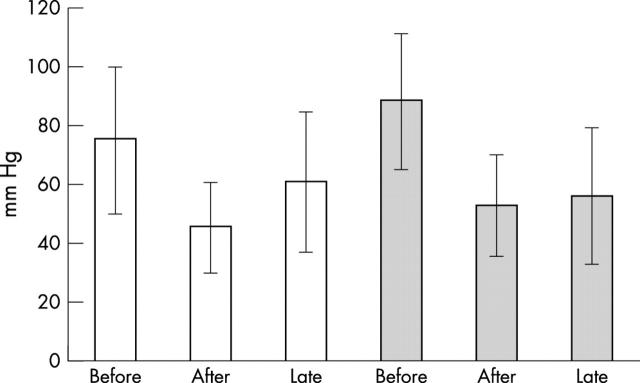
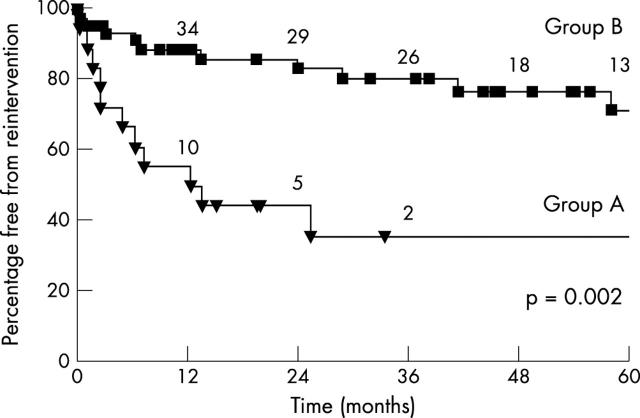
Results: The pressure gradient dropped significantly with the intervention and increased mildly at follow up. Freedom from relevant aortic regurgitation (that is, moderate and severe) was initially lower in group A (75% v 90% after one month) but after two years the difference between the two groups was not significant (50% v 61%). Freedom from reintervention was significantly lower in group A (with 35% v 80%) after three years.
Conclusion: Aortic balloon valvoplasty is safe and effective but has a high rate of early reintervention in infants with critical aortic stenosis. The major long term problem is progressive aortic regurgitation, which does not seem to be prevented by the use of small balloons.
Figures

Comment in
-
Management of valvar aortic stenosis in children.Heart. 2004 Jan;90(1):5-6. doi: 10.1136/heart.90.1.5. Heart. 2004. PMID: 14676226 Free PMC article.
References
-
- Rocchini AP, Beekman RH, Ben Shachar G, et al. Balloon aortic valvuloplasty: results of the valvuloplasty and angioplasty of congenital anomalies registry. Am J Cardiol 1990;65:784–9. - PubMed
-
- Justo RN, McCrindle BW, Benson LN, et al. Aortic valve regurgitation after surgical versus percutaneous balloon valvotomy for congenital aortic valve stenosis. Am J Cardiol 1996;77:1332–8. - PubMed
-
- Hawkins JA, Minich LL, Shaddy RE, et al. Aortic valve repair and replacement after balloon aortic valvuloplasty in children. Ann Thorac Surg 1996;61:1355–8. - PubMed
-
- Bacha EA, Satou GM, Moran AM, et al. Valve-sparing operation for balloon-induced aortic regurgitation in congenital aortic stenosis. J Thorac Cardiovasc Surg 2001;122:162–8. - PubMed
-
- Sholler GF, Keane JF, Perry SB, et al. Balloon dilatation of congenital aortic valve stenosis. Circulation 1988;78:351–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources