

Immunopathogenic mechanisms in psoriasis
- PMID: 14678257
- PMCID: PMC1808928
- DOI: 10.1111/j.1365-2249.2004.02310.x
Immunopathogenic mechanisms in psoriasis
Abstract
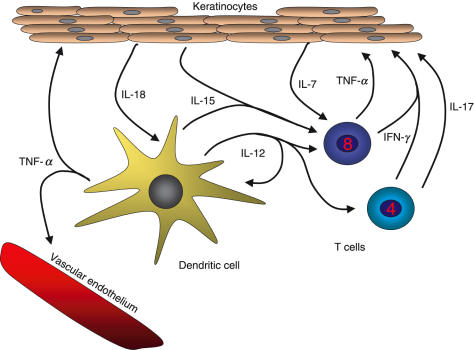
Psoriasis is a common autoimmune skin disease characterized by T cell-mediated hyperproliferation of keratinocytes. The disease has a strong but complex genetic background with a concordance of approximately 60% in monozygotic twins, and recent linkage and high resolution association studies indicate that HLA-Cw*0602 is itself a major susceptibility allele for psoriasis. Patients carrying this allele have been shown to have different clinical features and earlier age of disease onset, and patients homozygous for this allele have about 2.5 times higher disease risk than heterozygotes. Published data indicate that CD8+ T cells may play a major effector role in psoriasis. Epidermal infiltration of predominantly oligoclonal CD8+ T cells, and probably also of CD4+ T cells in the dermis, is a striking feature of chronic psoriasis lesions, indicating that these cells are responding to specific antigens. We argue that CD4+ T cells are essential for initiating and maintaining the pathogenic process of psoriasis but that cross-primed CD8+ T cells are the main effector cells responding to antigens in the HLA-Cw*0602 binding pocket of keratinocytes. It is further proposed that CD8+ T cells are involved in the control of the Th1 polarization, which is observed in psoriasis lesions, through a complex interplay between CD4+, CD8+ T cells and cross-presenting dendritic cells. It is also suggested that spontaneous remissions or fluctuations in disease activity may be determined by a balance within the lesions between effector and suppressor CD4+ and CD8+ T cells.
Figures


References
-
- Espinoza LR, Cuellar ML, Silveira LH. Psoriatic arthritis. Curr Opin Rheumatol. 1992;4:470–8. - PubMed
-
- Brandrup F, Holm N, Grunnet N, et al. Psoriasis in monozygotic twins: variations in expression in individuals with identical constitution. Acta Derma Venereol. 1982;62:229–36. - PubMed
-
- Gudjonsson JE, Karason A, Antonsdottir AA, et al. HLA-Cw6-Positive and HLA-Cw6-Negative Patients with Psoriasis Vulgaris have Distinct Clinical Features. J Invest Dermatol. 2002;118:362–5. - PubMed
-
- Enerback C, Martinsson T, Inerot A, et al. Evidence that HLA-Cw6 determines early onset of psoriasis, obtained using sequence-specific primers (PCR-SSP) Acta Derm Venereol. 1997;77:273–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
