

Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspective for an old disease
- PMID: 14685093
- PMCID: PMC1356185
- DOI: 10.1097/01.sla.0000102989.54824.fc
Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspective for an old disease
Abstract
Background: The Roux-en-Y gastric bypass and the biliopancreatic diversion effectively induce weight loss and long-term control of type 2 diabetes in morbidly obese individuals. It is unknown whether the control of diabetes is a secondary outcome from the treatment of obesity or a direct result of the duodenal-jejunal exclusion that both operations include. The aim of this study was to investigate whether duodenal-jejunal exclusion can control diabetes independently on resolution of obesity-related abnormalities.
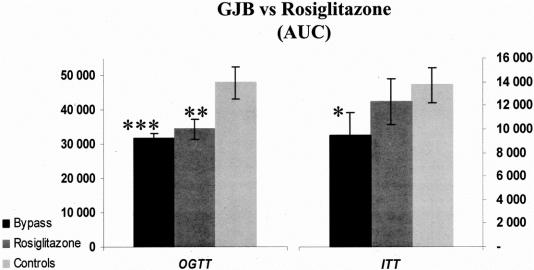
Methods: A gastrojejunal bypass (GJB) with preservation of an intact gastric volume was performed in 10- to 12-week-old Goto-Kakizaki rats, a spontaneous nonobese model of type 2 diabetes. Fasting glycemia, oral glucose tolerance, insulin sensitivity, basal plasma insulin, and glucose-dependent-insulinotropic peptide as well as plasma levels of cholesterol, triglycerides, and free fatty acids were measured. The GJB was challenged against a sham operation, marked food restriction, and medical therapy with rosiglitazone in matched groups of animals. Rats were observed for 36 weeks after surgery.
Results: Mean plasma glucose 3 weeks after GJB was 96.3 +/- 10.1 mg/dL (preoperative values were 159 +/- 47 mg/dL; P = 0.01). GJB strikingly improved glucose tolerance, inducing a greater than 40% reduction of the area under blood glucose concentration curve (P < 0.001). These effects were not seen in the sham-operated animals despite similar operative time, same postoperative food intake rates, and no significant difference in weight gain profile. GJB resulted also in better glycemic control than greater weight loss from food restriction and than rosiglitazone therapy.
Conclusions: Results of our study support the hypothesis that the bypass of duodenum and jejunum can directly control type 2 diabetes and not secondarily to weight loss or treatment of obesity. These findings suggest a potential role of the proximal gut in the pathogenesis the disease and put forward the possibility of alternative therapeutic approaches for the management of type 2 diabetes.
Figures





Comment in
-
Diabetes: the evolution of a new paradigm.Ann Surg. 2004 Jan;239(1):12-3. doi: 10.1097/01.sla.0000102990.47956.98. Ann Surg. 2004. PMID: 14685094 Free PMC article.
-
Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspective for an old disease.Ann Surg. 2004 Aug;240(2):388-9; author reply 389-91. doi: 10.1097/01.sla.0000134632.08789.df. Ann Surg. 2004. PMID: 15273570 Free PMC article. No abstract available.
References
-
- Venkat Narayan KM, Gregg EW, Fagot-Campagna A, et al. Diabetes—a common, growing, serious, costly, and potentially preventable public health problem. Diabetes Res Clin Pract. 2000;50(Suppl 2):S77–S784. - PubMed
-
- King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care. 1998;21:1414–1431. - PubMed
-
- Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414:782–787. - PubMed
-
- Brolin RE. Update: NIH consensus conference. Gastrointestinal surgery for severe obesity. Nutrition. 1996;12:403–404. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
