

Reductive surgery plus percutaneous isolated hepatic perfusion for multiple advanced hepatocellular carcinoma
- PMID: 14685100
- PMCID: PMC1356192
- DOI: 10.1097/01.sla.0000103133.03688.3d
Reductive surgery plus percutaneous isolated hepatic perfusion for multiple advanced hepatocellular carcinoma
Abstract
Objective: To evaluate the efficacy of a novel 2-stage treatment with reductive surgery plus percutaneous isolated hepatic perfusion (PIHP) for multiple hepatocellular carcinoma (HCC), which was previously unresectable.
Summary background data: Surgical resection is the treatment of choice for HCC, but the majority of patients with advanced HCC are not suitable candidates. PIHP is a minimally invasive surgery that allows high-dose regional chemotherapy of the liver, and our phase II studies have shown its profound efficacy for the local control of advanced HCC.
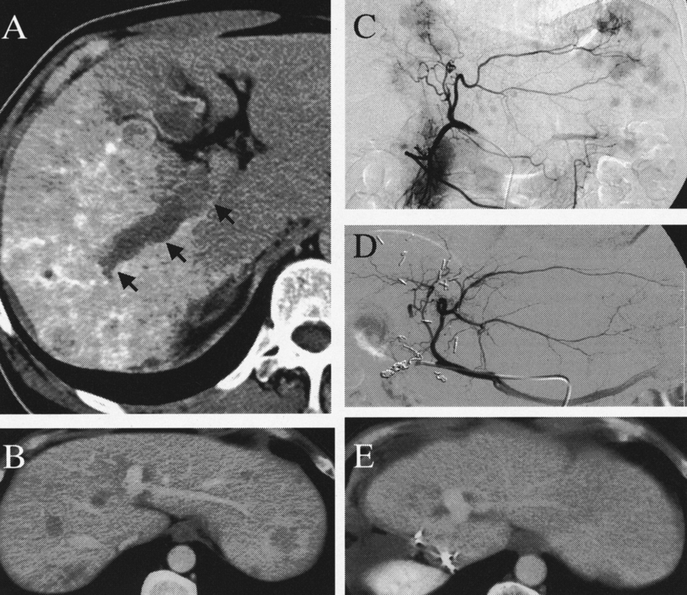
Methods: Twenty-five patients with multiple advanced HCC were enrolled in this prospective study. In the first stage, all patients underwent reductive hepatectomy: major hepatectomy in 13 patients and segmentectomy or less in 12. In 2 patients with subsegmentectomy, the retropancreatic and periportal metastatic lymph nodes were synchronously resected. Regardless of the type of hepatectomy, all patients routinely underwent cholecystectomy, and ligations of the right gastric artery and arterial collaterals of the remnant liver to increase the safety and efficacy of PIHP. In the second stage, PIHP with doxorubicin 60-120 mg/m2/treatment was planned for a period of 1 to 3 months after surgery.
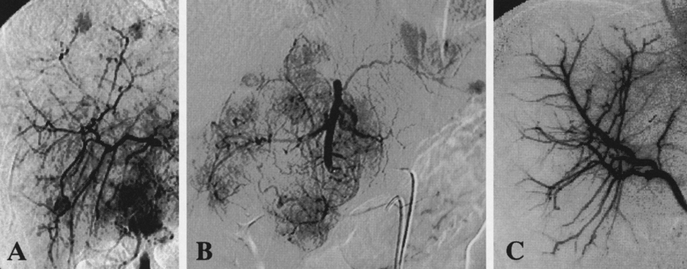
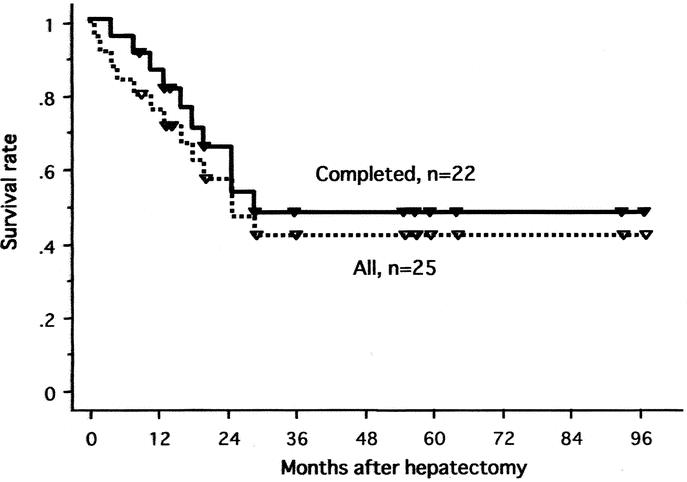
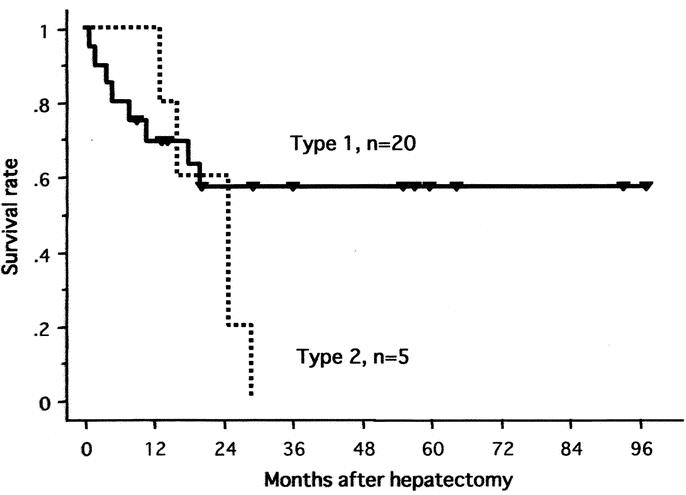
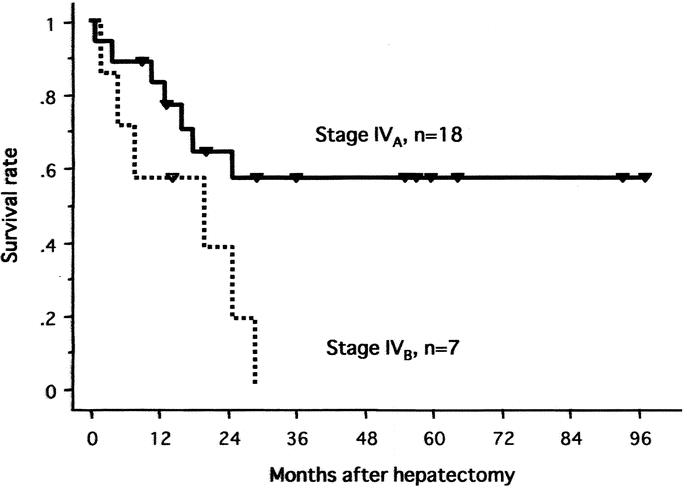
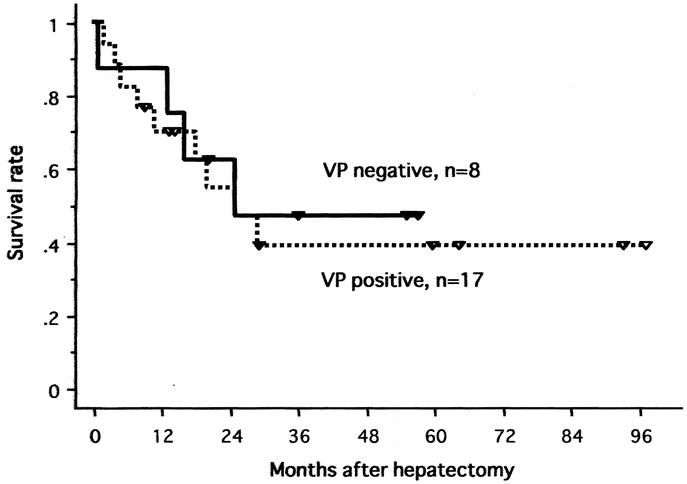
Results: Of 25 enrolled patients, 22 successfully underwent PIHP an average of 1.8 times for the local control of residual liver tumors. In the remaining 3 patients, PIHP was abandoned because 2 had rapid disease progression and 1 had liver failure after surgery. In 22 patients with the 2-stage treatment, 19 (86%) had objective local tumor control (10 complete remissions and 9 partial responses with a median response duration of 16 months). The actuarial survival rate of all 25 patients was 42% at 5 years.
Conclusions: Reductive surgery plus PIHP produced a strong antitumoral effect on multiple advanced HCC, when liver function allows this concentrated treatment approach, and offers long-term survival in a subset of patients who were previously deemed to have unresectable disease.
Figures
References
-
- Mor E, Tur Kaspa R, Sheiner P, et al. Treatment of hepatocellular carcinoma associated with cirrhosis in the era of liver transplantation. Ann Intern Med. 1998;129:643–653. - PubMed
-
- Bismuth H, Houssin D, Ornowski J, et al. Liver resections in cirrhotic patients: a Western experience. World J Surg. 1986;10:311–317. - PubMed
-
- Sasaki Y, Imaoka S, Masutani S, et al. Influence of coexisting cirrhosis on long-term prognosis after surgery in patients with hepatocellular carcinoma. Surgery. 1992;112:515–512. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
