

Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life
- PMID: 14685109
- PMCID: PMC1356201
- DOI: 10.1097/01.sla.0000103067.10695.74
Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life
Abstract
Objective: We evaluated the long-term impact of iliofemoral thrombosis (I-FDVT) on walking capacity, venous hemodynamic status, CEAP class, venous clinical severity, and quality of life, and determined the prevalence of venous claudication.
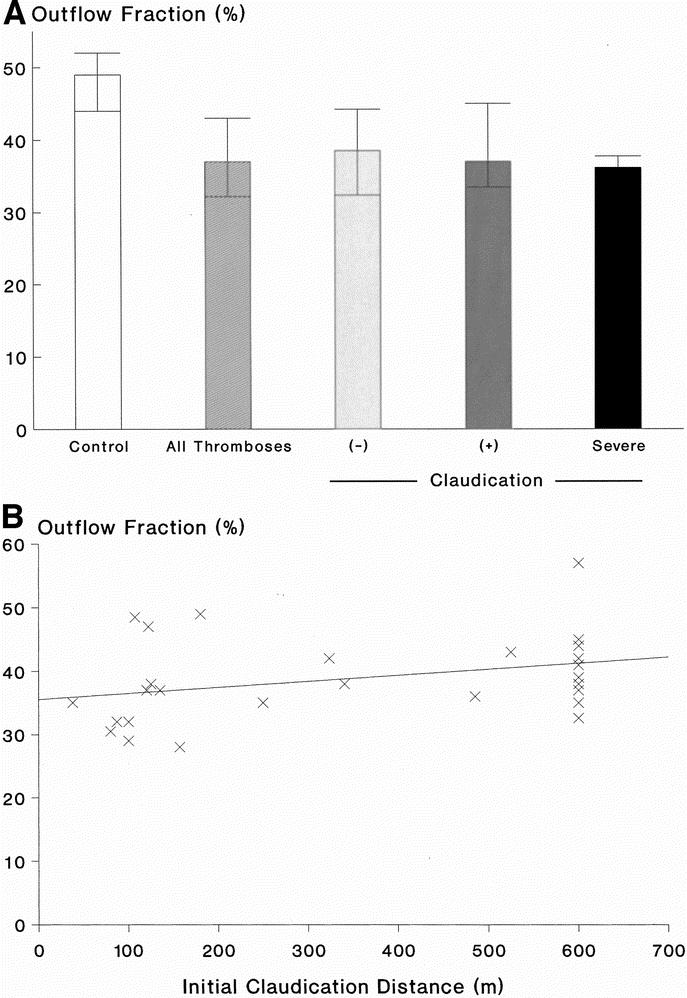
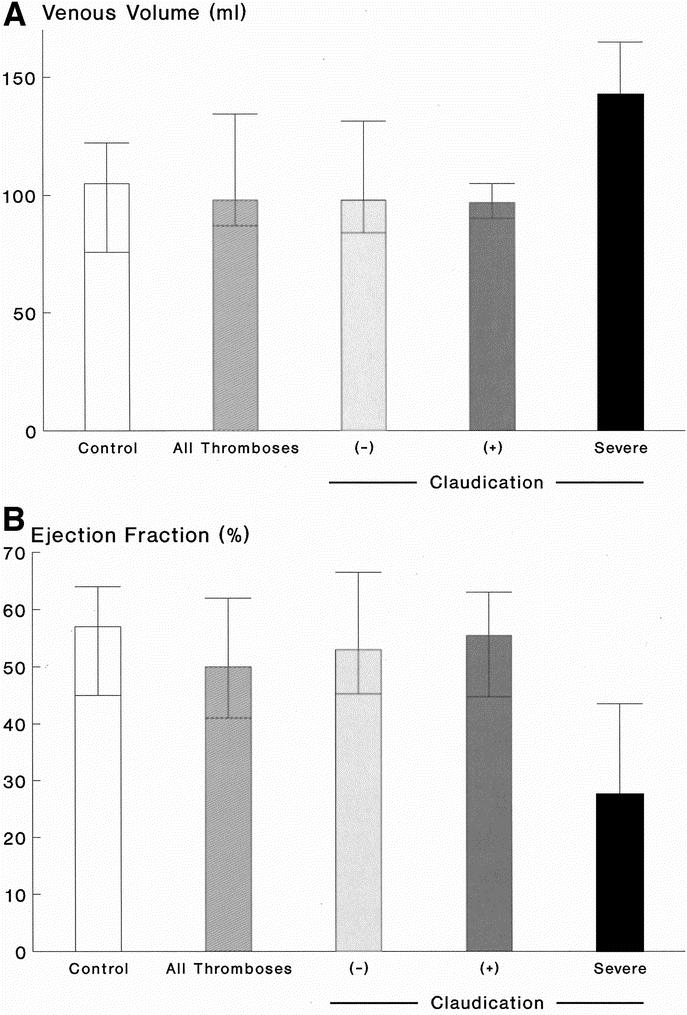
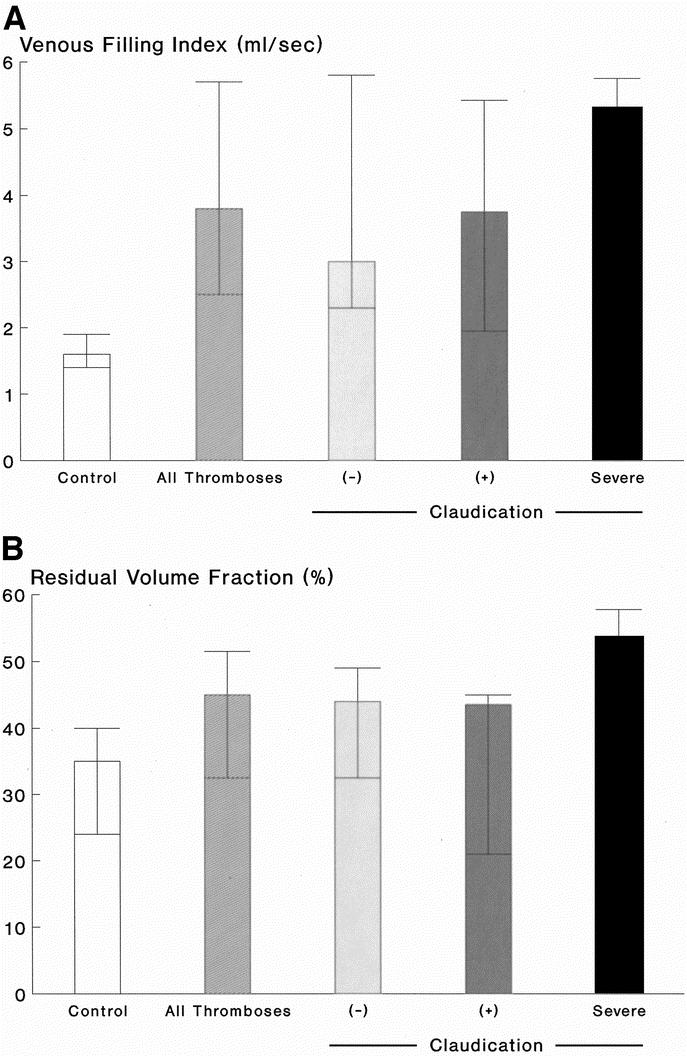
Materials and methods: All patients with prior I-FDVT, assessed at our institution since 1990, were called for follow-up. Those with walking impairment due to arterial disease (ABI < 1.0 postexercise) or unrelated causes and those thrombectomized or thrombolyzed were excluded; 39 patients (22-83 years, median 46 years) were included. Median follow-up was 5 years (range 1-23 years). Investigation included classification in CEAP and Venous Clinical Severity Scoring (VCSS) systems, air-plethysmography (outflow fraction [OF], venous filling index [VFI], residual volume fraction [RVF]) and venous duplex, treadmill (3.5 km/h, 10%) to determine initial (ICD) and absolute (ACD) claudication distances, and quality of life assessment (SF-36). Nonaffected limbs of patients with unilateral I-FDVT (37 of 39) comprised the control group. Data are presented as median and interquartile range.
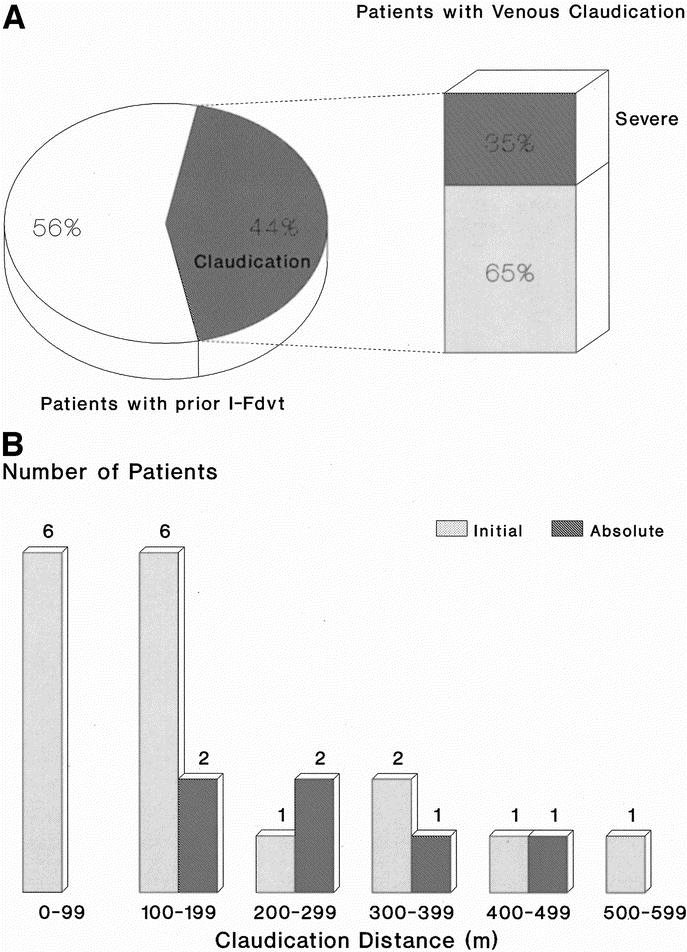
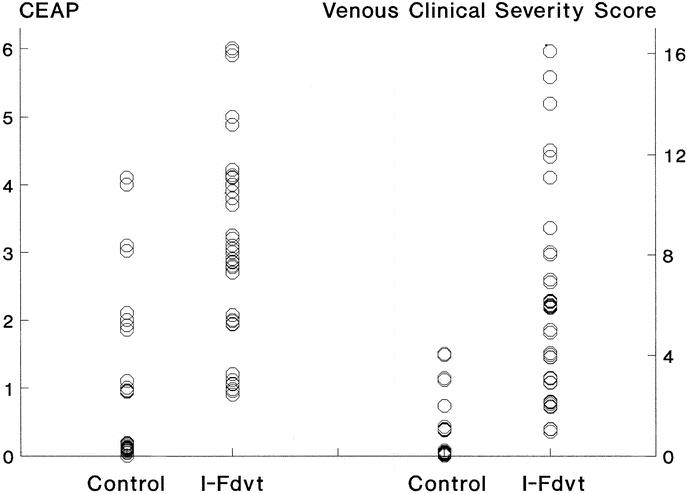
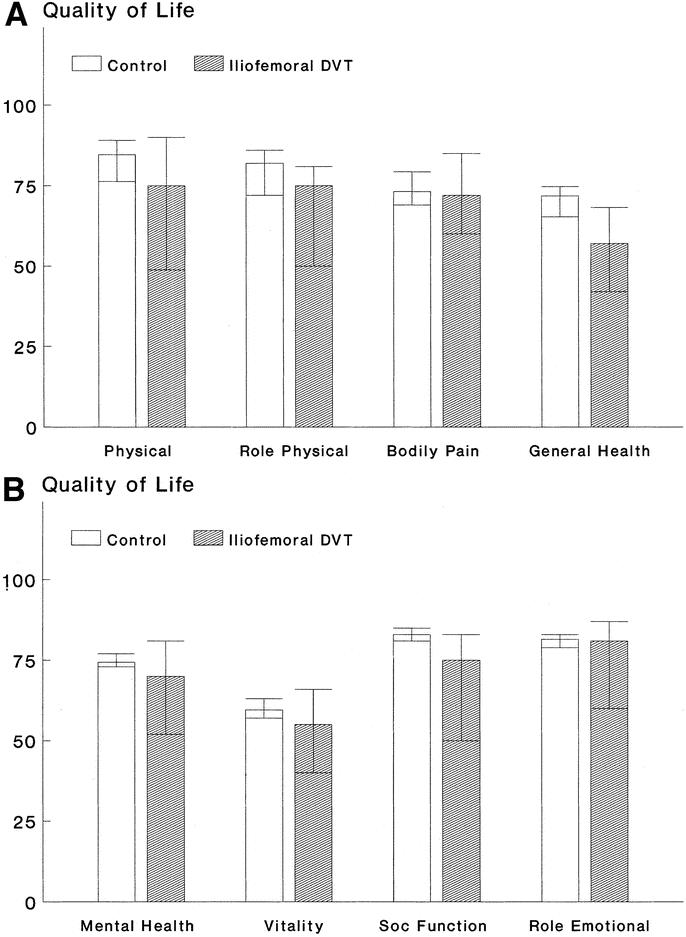
Results: A total of 81% of limbs with I-FDVT had superficial and deep reflux and 19% superficial reflux; reflux in control limbs was 29.7% (P < 0.001) and 27% (P > 0.2), respectively; 43.6% (17 of 39; 95% CI, 27-60%) of patients developed venous claudication ipsilateral to I-FDVT (ICD: 130 m, range 105-268 m), compelling 15.4% (6 of 39; 95% CI, 3.5-27%) to discontinue treadmill (ACD: 241 m, range 137-298 m). Limbs with prior I-FDVT had a lower OF (37%, range 32.2-43%; P < 0.001), abnormally higher VFI (3.8 mL/s, range 2.5-5.7 mL/s; P < 0.001), and RVF (45%, range 32.5-51.5%; P = 0.006), and clinical impairment in CEAP and VCSS systems (P < 0.0001). Patients with I-FDVT had impaired physical functioning (P = 0.02) and role (P = 0.033), general health (P = 0.001), social function (P = 0.047), and mental health (P = 0.043).
Conclusions: A total of 43.6% of those with prior I-FDVT developed venous claudication compelling interruption of walking in 15.4%. Prior I-FDVT caused outflow impairment and a large residual venous volume and reflux, resulting in marked clinical and quality of life compromise. Standardized challenge enabled discrimination of those with clinically relevant impairment.
Figures
References
-
- Gjores JE. The incidence of venous thrombosis and its sequelae in certain districts of Sweden. Acta Chir Scand. 1956;(suppl 206). - PubMed
-
- Mavor GE, Galloway JM. Iliofemoral venous thrombosis: pathological considerations and surgical management. Br J Surg. 1969;56:45–59. - PubMed
-
- Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 19961;125:1–7. - PubMed
-
- Plate G, Eklof B, Norgren L, et al. Venous thrombectomy for iliofemoral vein thrombosis: 10-year results of a prospective randomised study. Eur J Vasc Endovasc Surg. 1997;14:367–374. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
