

A randomized comparison of patients' understanding of number needed to treat and other common risk reduction formats
- PMID: 14687273
- PMCID: PMC1494938
- DOI: 10.1046/j.1525-1497.2003.21102.x
A randomized comparison of patients' understanding of number needed to treat and other common risk reduction formats
Abstract
Background: Commentators have suggested that patients may understand quantitative information about treatment benefits better when they are presented as numbers needed to treat (NNT) rather than as absolute or relative risk reductions.
Objective: To determine whether NNT helps patients interpret treatment benefits better than absolute risk reduction (ARR), relative risk reduction (RRR), or a combination of all three of these risk reduction presentations (COMBO).
Design: Randomized cross-sectional survey.
Setting: University internal medicine clinic.
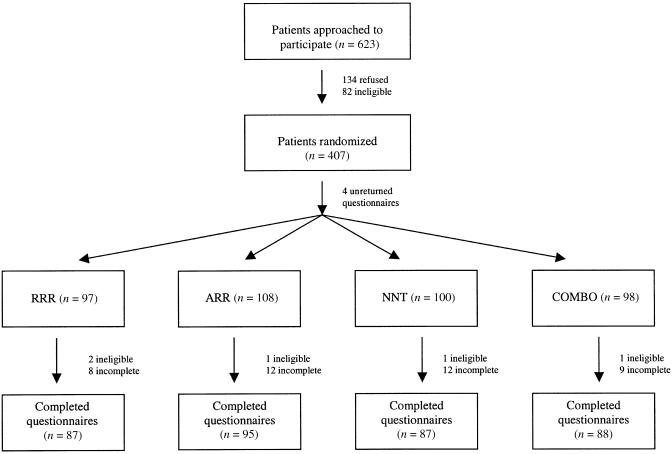
Patients: Three hundred fifty-seven men and women, ages 50 to 80, who presented for health care.
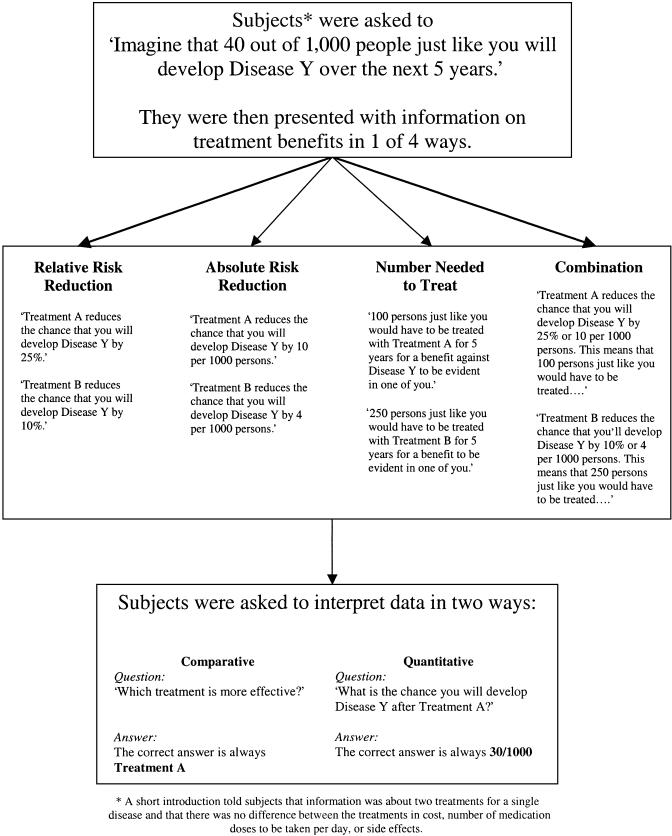
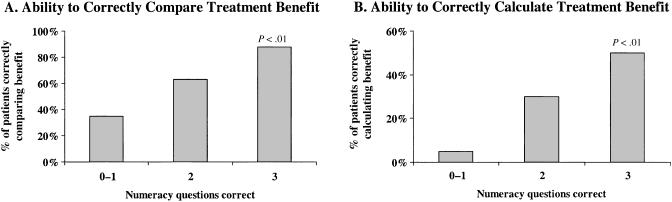
Interventions: Subjects were given written information about the baseline risk of a hypothetical "disease Y" and were asked (1) to compare the benefits of two drug treatments for disease Y, stating which provided more benefit; and (2) to calculate the effect of one of those drug treatments on a given baseline risk of disease. Risk information was presented to each subject in one of four randomly allocated risk formats: NNT, ARR, RRR, or COMBO.
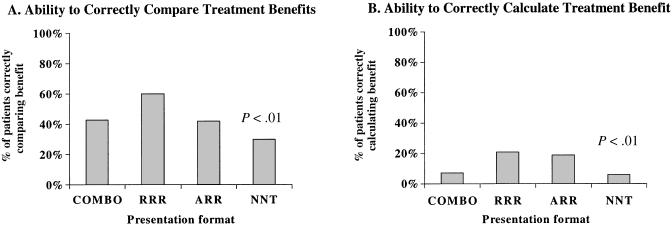
Main results: When asked to state which of two treatments provided more benefit, subjects who received the RRR format responded correctly most often (60% correct vs 43% for COMBO, 42% for ARR, and 30% for NNT, P =.001). Most subjects were unable to calculate the effect of drug treatment on the given baseline risk of disease, although subjects receiving the RRR and ARR formats responded correctly more often (21% and 17% compared to 7% for COMBO and 6% for NNT, P =.004).
Conclusion: Patients are best able to interpret the benefits of treatment when they are presented in an RRR format with a given baseline risk of disease. ARR also is easily interpreted. NNT is often misinterpreted by patients and should not be used alone to communicate risk to patients.
Figures
Comment in
-
Why does framing influence judgment?J Gen Intern Med. 2003 Nov;18(11):960-1. doi: 10.1046/j.1525-1497.2003.30901.x. J Gen Intern Med. 2003. PMID: 14687283 Free PMC article. No abstract available.
References
-
- Institute of Medicine (US). Envisioning the National Health Care Quality Report. Washington, DC: The Institute; 2001.
-
- Rajkumar S, Sampathkumar P, Gustafson A. Number needed to treat is a simple measure of treatment efficacy for clinicians. J Gen Intern Med. 1996;11:357–9. - PubMed
-
- Schwartz LM, Woloshin S, Black WC, Welch HG. The role of numeracy in understanding the benefit of screening mammography. Ann Intern Med. 1997;127:966–72. - PubMed
-
- Laupacis A, Sackett D, Roberts R. An assessment of clinically useful measures of the consequences of treatment. N Engl J Med. 1988;318:1728–33. - PubMed
-
- Sackett D. Inference and decision at the bedside. J Clin Epidemiol. 1989;42:309–16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources