

African American church participation and health care practices
- PMID: 14687276
- PMCID: PMC1494942
- DOI: 10.1046/j.1525-1497.2003.20936.x
African American church participation and health care practices
Abstract
Background: While religious involvement is associated with improvements in health, little is known about the relationship between church participation and health care practices.
Objectives: To determine 1) the prevalence of church participation; 2) whether church participation influences positive health care practices; and 3) whether gender, age, insurance status, and levels of comorbidity modified these relationships.
Design: A cross-sectional analysis using survey data from 2196 residents of a low-income, African-American neighborhood.
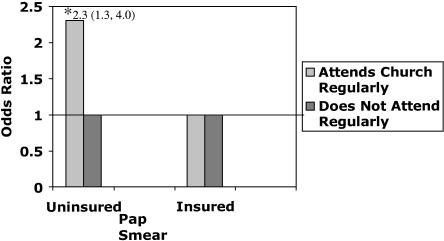
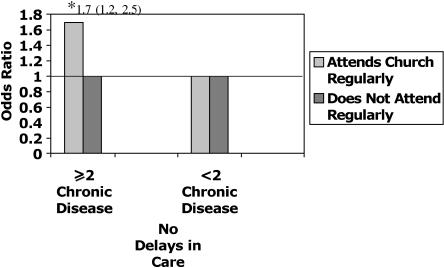
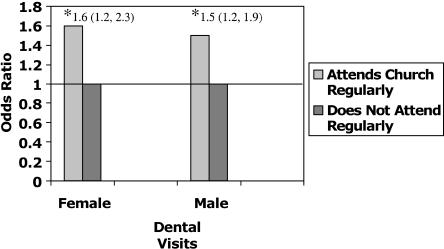
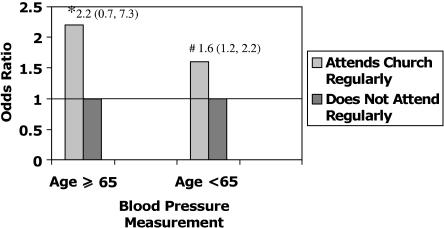
Measurements: Our independent variable measured the frequency of church attendance. Dependent variables were: 1) Pap smear; 2) mammogram; and 3) dental visit-all taking place within 2 years; 4) blood pressure measurement within 1 year, 5) having a regular source of care, and 6) no perceived delays in care in the previous year. We controlled for socioeconomic factors and the number of comorbid conditions and also tested for interactions.
Results: Thirty-seven percent of community members went to church at least monthly. Church attendance was associated with increased likelihood of positive health care practices by 20% to 80%. In multivariate analyses, church attendance was related to dental visits (odds ratio [OR], 1.5; 95% confidence interval [CI], 1.3 to 1.9) and blood pressure measurements (OR, 1.6; 95% CI, 1.2 to 2.1). Insurance status and number of comorbid conditions modified the relationship between church attendance and Pap smear, with increased practices noted for the uninsured (OR, 2.3; 95% CI, 1.2 to 4.1) and for women with 2 or more comorbid conditions (OR, 1.9; 95% CI, 1.1 to 3.5).
Conclusion: Church attendance is an important correlate of positive health care practices, especially for the most vulnerable subgroups, the uninsured and chronically ill. Community- and faith-based organizations present additional opportunities to improve the health of low-income and minority populations.
Figures
Comment in
-
Health care and faith communities: how are they related?J Gen Intern Med. 2003 Nov;18(11):962-3. doi: 10.1046/j.1525-1497.2003.30902.x. J Gen Intern Med. 2003. PMID: 14687284 Free PMC article. No abstract available.
References
-
- Chatters LM, Levin JS, Ellison CG. Public health and health education in faith communities. Health Educ Behav. 1998;25:689–99. - PubMed
-
- Chatters LM. Religion and health: public health research and practice. Annu Rev Public Health. 2000;21:335–67. - PubMed
-
- Campbell MK, Motsinger BM, Ingram A, et al. The North Carolina Black Churches United for Better Health Project: intervention and process evaluation. Health Educ Behav. 2000;27:241–53. - PubMed
-
- Gallant MP, Dorn GP. Gender and race differences in the predictors of daily health practices among older adults. Health Educ Res. 2001;16:21–31. - PubMed
-
- Hummer RA, Rogers RG, Nam CB, Ellison CG. Religious involvement and U.S. adult mortality. Demography. 1999;36:273–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials