

Comparative Study
doi: 10.1128/AAC.48.1.340-343.2004.
In vitro postantibiotic effects of rifapentine, isoniazid, and moxifloxacin against Mycobacterium tuberculosis
Affiliations
- PMID: 14693563
- PMCID: PMC310201
- DOI: 10.1128/AAC.48.1.340-343.2004
Item in Clipboard
Comparative Study
In vitro postantibiotic effects of rifapentine, isoniazid, and moxifloxacin against Mycobacterium tuberculosis
Antimicrob Agents Chemother.
2004 Jan.
Abstract
Postantibiotic effects (PAEs) of rifapentine, isoniazid, and moxifloxacin against Mycobacterium tuberculosis ATCC 27294 were studied using a radiometric culture system. Rifapentine at 20 mg/liter gave the longest PAE (104 h) among the drugs used alone. The combinations of rifapentine plus isoniazid, rifapentine plus moxifloxacin, and isoniazid plus moxifloxacin gave PAEs of 136.5, 59.0, and 8.3 h, respectively.
Figures
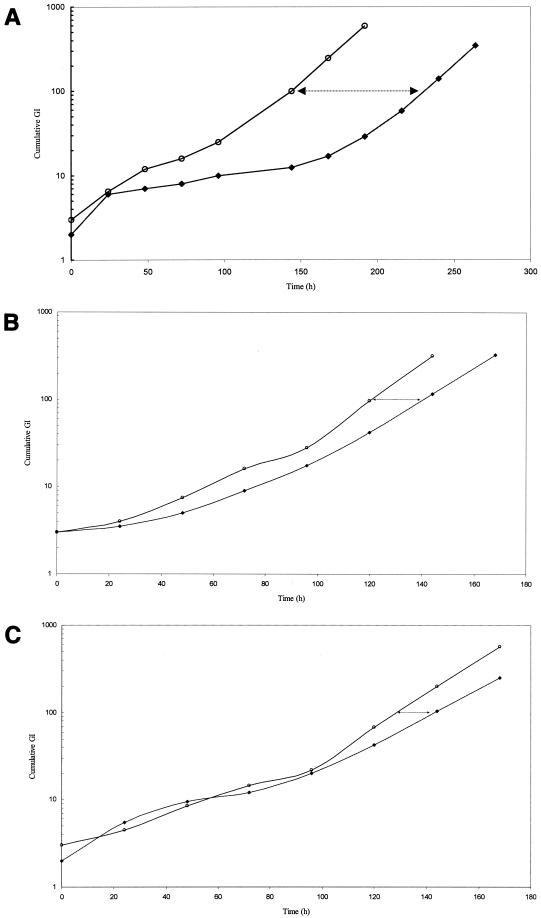
(A) Regrowth curves of M. tuberculosis H37Rv following 2 h of exposure to rifapentine (10 mg/liter). ○, cumulative GI of residual control; ♦, cumulative GI of exposed culture. The time interval between cumulative GI lines (arrows) denotes the PAE. (B) Regrowth curves of M. tuberculosis H37Rv following 2 h of exposure to isoniazid (2 mg/liter). ○, cumulative GI of residual control; ♦, cumulative GI of exposed culture. The time interval between the lines (arrows) denotes the PAE. (C) Regrowth curves of M. tuberculosis H37Rv following 2 h of exposure to moxifloxacin (2 mg/liter). ○, cumulative GI of residual control; ♦, cumulative GI of exposed culture. The time interval between the lines (arrows) denotes the PAE.
References
-
- Benator, D., M. Bhattacharya, L. Bozeman, W. Burman, A. Cantazaro, R. Chaisson, F. Gordin, C. R. Horsburgh, J. Horton, A. Khan, C. Lahart, B. Metchock, C. Pachucki, L. Stanton, A. Vernon, M. E. Villarino, Y. C. Wang, M. Weiner, S. Weis, et al. 2002. Rifapentine and isoniazid once a week versus rifampicin and isoniazid twice a week for treatment of drug-susceptible pulmonary tuberculosis in HIV-negative patients: a randomised clinical trial. Lancet 360:528-534. - PubMed
-
- Bock, N. N., T. R. Sterling, C. D. Hamilton, C. Pachucki, Y. C. Wang, D. S. Conwell, A. Mosher, M. Samuels, A. Vernon, et al. 2002. A prospective, randomized, double-blind study of the tolerability of rifapentine 600, 900, and 1,200 mg plus isoniazid in the continuation phase of tuberculosis treatment. Am. J. Resp. Crit. Care Med. 165:1526-1530. - PubMed
-
- Bundtzen, R. W., A. U. Gerber, D. L. Cohn, and W. A. Craig. 1981. Post-antibiotic suppression of bacterial growth. Rev. Infect. Dis. 3:28-37. - PubMed
-
- Burkhardt, O., K. Borner, H. Stass, G. Beyer, M. Allewelt, C. E. Nord, and H. Lode. 2002. Single- and multiple-dose pharmacokinetics of oral moxifloxacin and clarithromycin, and concentrations in serum, saliva and faeces. Scand. J. Infect. Dis. 34:898-903. - PubMed
-
- Burman, W. J., K. Gallicano, and C. Peloquin. 2001. Comparative pharmacokinetics and pharmacodynamics of the rifamycin antibacterials. Clin. Pharmacokinet. 40:327-341. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
