

Is cost-effectiveness analysis preferred to severity of disease as the main guiding principle in priority setting in resource poor settings? The case of Uganda
- PMID: 14711374
- PMCID: PMC324572
- DOI: 10.1186/1478-7547-2-1
Is cost-effectiveness analysis preferred to severity of disease as the main guiding principle in priority setting in resource poor settings? The case of Uganda
Abstract
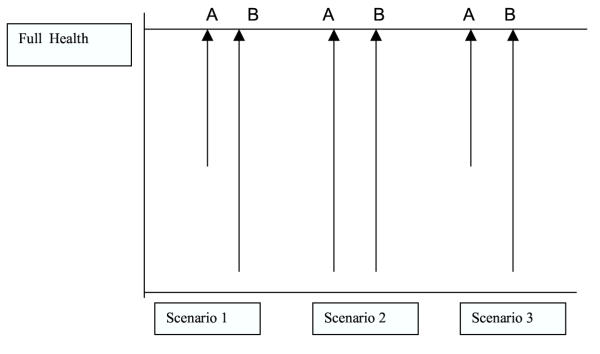
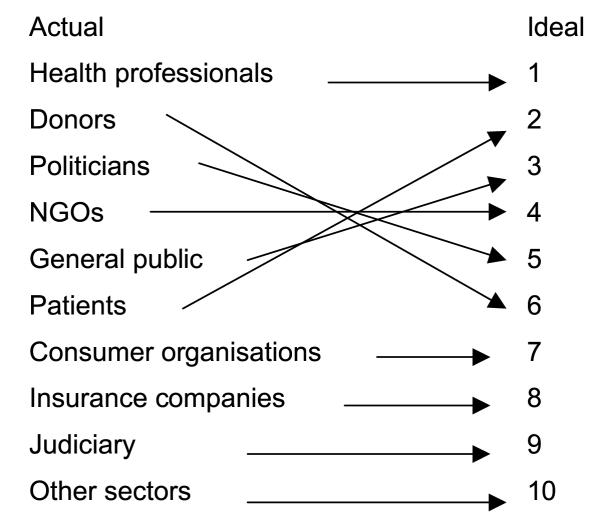
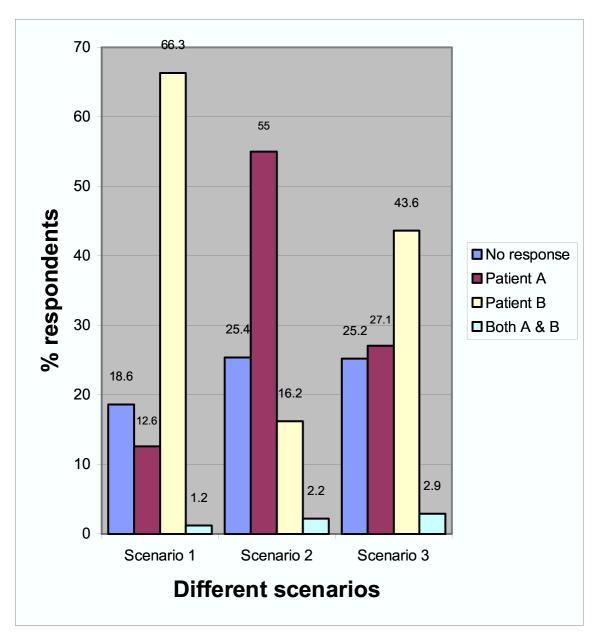
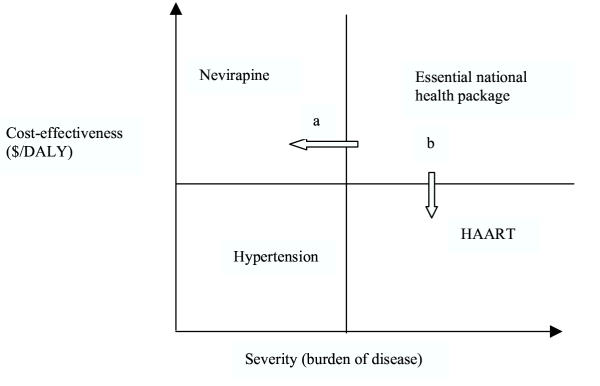
INTRODUCTION: Several studies carried out to establish the relative preference of cost-effectiveness of interventions and severity of disease as criteria for priority setting in health have shown a strong preference for severity of disease. These preferences may differ in contexts of resource scarcity, as in developing countries, yet information is limited on such preferences in this context. OBJECTIVE: This study was carried out to identify the key players in priority setting in health and explore their relative preference regarding cost-effectiveness of interventions and severity of disease as criteria for setting priorities in Uganda. DESIGN: 610 self-administered questionnaires were sent to respondents at national, district, health sub-district and facility levels. Respondents included mainly health workers. We used three different simulations, assuming same patient characteristics and same treatment outcome but with varying either severity of disease or cost-effectiveness of treatment, to explore respondents' preferences regarding cost-effectiveness and severity. RESULTS: Actual main actors were identified to be health workers, development partners or donors and politicians. This was different from what respondents perceived as ideal. Above 90% of the respondents recognised the importance of both severity of disease and cost-effectiveness of intervention. In the three scenarios where they were made to choose between the two, a majority of the survey respondents assigned highest weight to treating the most severely ill patient with a less cost-effective intervention compared to the one with a more cost-effective intervention for a less severely ill patient. However, international development partners in in-depth interviews preferred the consideration of cost-effectiveness of intervention. CONCLUSIONS: In a survey among health workers and other actors in priority setting in Uganda, we found that donors are considered to have more say than the survey respondents found ideal. Survey respondents considered both severity of disease and cost-effectiveness important criteria for setting priorities, with severity of disease as the leading principle. This pattern of preferences is similar to findings in context with relatively more resources. In-depth interviews with international development partners, showed that this group put relatively more emphasis on cost-effectiveness of interventions compared to severity of disease. These discrepancies in attitudes between national health workers and representatives from the donors require more investigation. The different attitudes should be openly debated to ensure legitimate decisions.
Figures
References
-
- Nilstun T. Priority setting, justice, and health care: Conceptual analysis. Croatian medical journa. 2000;41: 375–377. - PubMed
-
- Martin DK, Singer PA. Priority setting and health technology assessment:beyond evidence-based medicine and cost-effectiveness analysis. In: Coulter A and Ham C, editor. The Global Challenge of Health Care rationing. Philadelphia, Open University Press; 2000. pp. 135–145.
-
- Coast J. Explicit rationing, deprivation disutility and denial disutility:evidence from a qualitative study. In: Coulter A and Ham C, editor. The Global Challenge of Health Care rationing. Philadelphia, Open University Press; 2000. pp. 192–200.
LinkOut - more resources
Full Text Sources
