

Expression of co-stimulator 4-1BB molecule in hepatocellular carcinoma and adjacent non-tumor liver tissue, and its possible role in tumor immunity
- PMID: 14716821
- PMCID: PMC4717002
- DOI: 10.3748/wjg.v10.i2.195
Expression of co-stimulator 4-1BB molecule in hepatocellular carcinoma and adjacent non-tumor liver tissue, and its possible role in tumor immunity
Abstract
Aim: To investigate the expression of 4-1BB molecule in hepatocellular carcinoma (HCC) and its adjacent tissues.
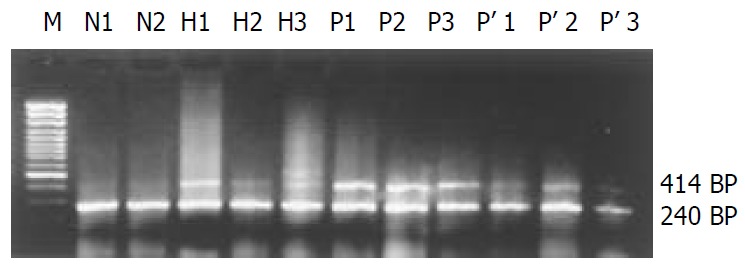
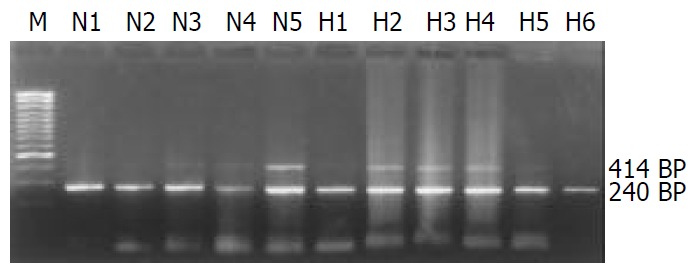
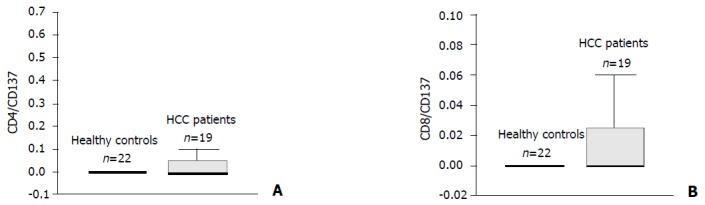
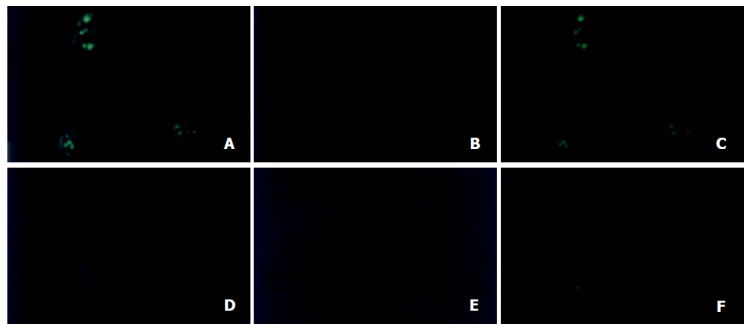
Methods: Reverse transcription-polymerase chain reaction (RT-PCR) was used to determine the gene expression of 4-1BB in hepatocarcinoma and its adjacent tissues, and peripheral blood mononuclear cells (PBMCs) from both HCC and health control groups. Flow cytometry was used to analyse the phenotypes of T cell subsets from the blood of HCC patients and healthy volunteers, and further to determine whether 4-1BB molecules were also expressed on the surface of CD4+ and CD8+ T cells. The localization of 4-1BB proteins on tumor infiltrating T cells was determined by direct immunofluorescence cytochemical staining and detected by confocal microscopy.
Results: 4-1BB mRNA, which was not detectable in normal liver, was found in 19 liver tissues adjacent to tumor edge (<1.0 cm). Low expression of 4-1BB mRNA was shown in 8 tumor tissues and 6 liver tissues located within 1 to 5 cm away from tumor edge. In PBMCs, 4-1BB mRNA was almost not detected. Percentage of CD4+, CD8+ and CD3+/CD25+ T cells, as well as ratio of CD4 to CD8 revealed no difference between groups (P>0.05, respectively), while a significant lower percentage of CD3+ T cell was found in HCC group as compared to healthy control group (P<0.05). However, 4-1BB molecules were almost not found on the surface of CD4+ and CD8+ T cells in HCC and healthy control group. Double-staining of 4-1BB+/CD4+ and 4-1BB+/CD8+ immunofluorescence on tumor infiltrating T cells was detected in 13 liver tissues adjacent to tumor edge (<1.0 cm) by confocal microscopy.
Conclusion: Although HCC may escape from immune attack by weak immunogenicity or downregulated expression of MHC-1 molecules on the tumor cell surface, tumor infiltrating T cells can be activated via other costimulatory signal pathways to exert a limited antitumor effect on local microenvironment. The present study also implicates that modulating 4-1BB/4-1BBL costimulatory pathway may be an effective immunotherapy strategy to augment the host response.
Figures
References
-
- Tang ZY, Yu YQ, Zhou XD, Ma ZC, Wu ZQ. Progress and prospects in hepatocellular carcinoma surgery. Ann Chir. 1998;52:558–563. - PubMed
-
- Kanematsu T, Furui J, Yanaga K, Okudaira S, Shimada M, Shirabe K. A 16-year experience in performing hepatic resection in 303 patients with hepatocellular carcinoma: 1985-2000. Surgery. 2002;131(1 Suppl):S153–S158. - PubMed
-
- Chiappa A, Zbar AP, Audisio RA, Leone BE, Biella F, Staudacher C. Factors affecting survival and long-term outcome in the cirrhotic patient undergoing hepatic resection for hepatocellular carcinoma. Eur J Surg Oncol. 2000;26:387–392. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
