

Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care
- PMID: 14724129
- PMCID: PMC324451
- DOI: 10.1136/bmj.37956.664236.EE
Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care
Abstract
Objectives: To measure the effectiveness and cost effectiveness of providing care in a chest pain observation unit compared with routine care for patients with acute, undifferentiated chest pain.
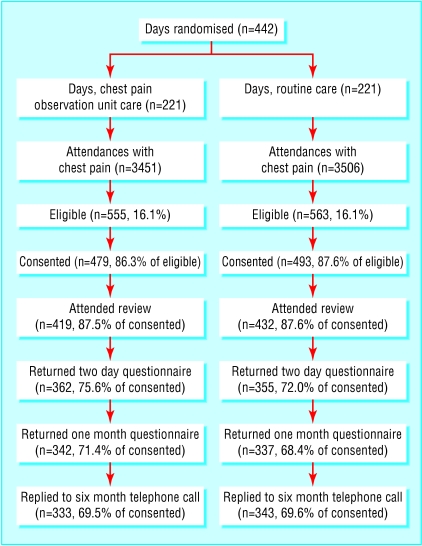
Design: Cluster randomised controlled trial, with 442 days randomised to the chest pain observation unit or routine care, and cost effectiveness analysis from a health service costing perspective.
Setting: The emergency department at the Northern General Hospital, Sheffield, United Kingdom.
Participants: 972 patients with acute, undifferentiated chest pain (479 attending on days when care was delivered in the chest pain observation unit, 493 on days of routine care) followed up until six months after initial attendance.
Main outcome measures: The proportion of participants admitted to hospital, the proportion with acute coronary syndrome sent home inappropriately, major adverse cardiac events over six months, health utility, hospital reattendance and readmission, and costs per patient to the health service.
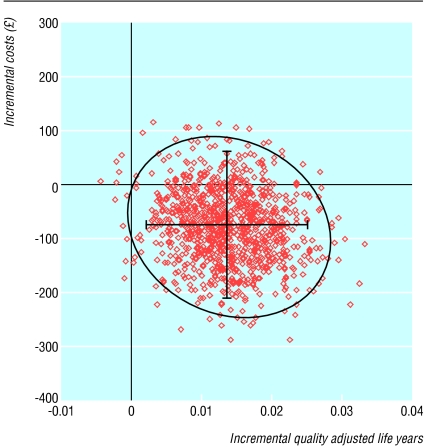
Results: Use of a chest pain observation unit reduced the proportion of patients admitted from 54% to 37% (difference 17%, odds ratio 0.50, 95% confidence interval 0.39 to 0.65, P < 0.001) and the proportion discharged with acute coronary syndrome from 14% to 6% (8%, -7% to 23%, P = 0.264). Rates of cardiac event were unchanged. Care in the chest pain observation unit was associated with improved health utility during follow up (0.0137 quality adjusted life years gained, 95% confidence interval 0.0030 to 0.0254, P = 0.022) and a saving of pound 78 per patient (- pound 56 to pound 210, P = 0.252).
Conclusions: Care in a chest pain observation unit can improve outcomes and may reduce costs to the health service. It seems to be more effective and more cost effective than routine care.
Figures
References
-
- Department of Health. The national service framework for coronary heart disease. London, DoH, 2000.
-
- Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL. The rational clinical examination. Is this patient having a myocardial infarction? JAMA 1998;280: 1256-63. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnosis of acute cardiac ischaemia in the emergency department. N Engl J Med 2000;342: 1163-70. - PubMed