

Multicentre, cluster-randomized clinical trial of algorithms for critical-care enteral and parenteral therapy (ACCEPT)
- PMID: 14734433
- PMCID: PMC315525
Multicentre, cluster-randomized clinical trial of algorithms for critical-care enteral and parenteral therapy (ACCEPT)
Abstract
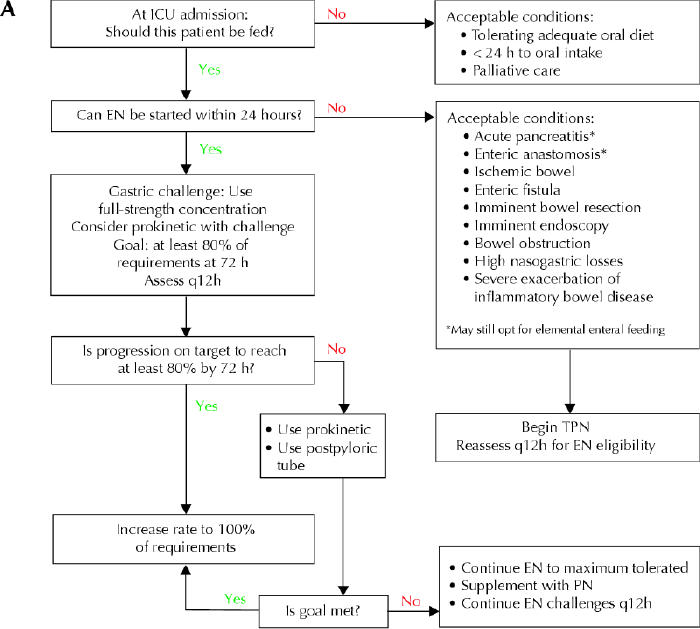
Background: The provision of nutritional support for patients in intensive care units (ICUs) varies widely both within and between institutions. We tested the hypothesis that evidence-based algorithms to improve nutritional support in the ICU would improve patient outcomes.
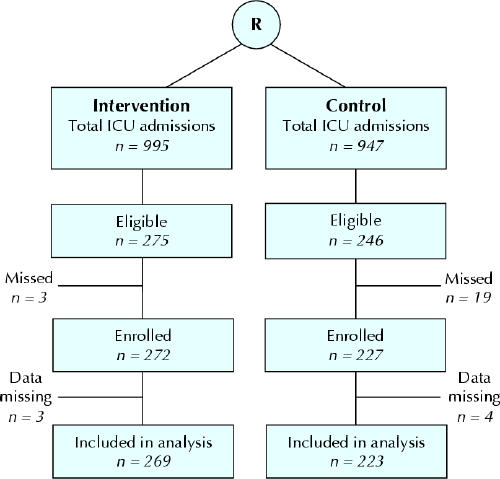
Methods: A cluster-randomized controlled trial was performed in the ICUs of 11 community and 3 teaching hospitals between October 1997 and September 1998. Hospital ICUs were stratified by hospital type and randomized to the intervention or control arm. Patients at least 16 years of age with an expected ICU stay of at least 48 hours were enrolled in the study (n = 499). Evidence-based recommendations were introduced in the 7 intervention hospitals by means of in-service education sessions, reminders (local dietitian, posters) and academic detailing that stressed early institution of nutritional support, preferably enteral.
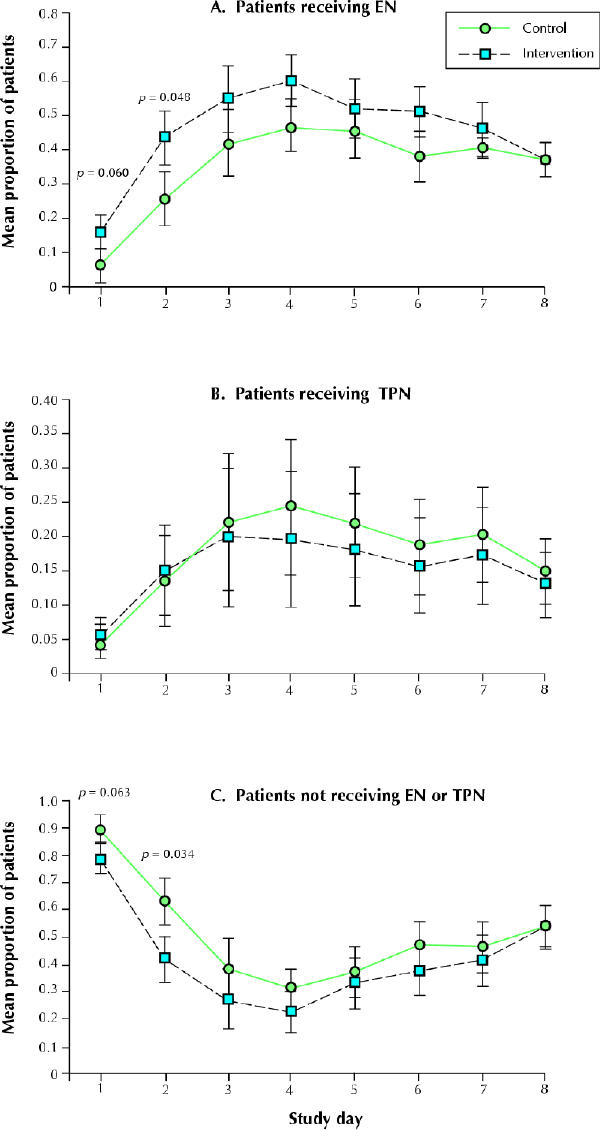
Results: Two hospitals crossed over and were excluded from the primary analysis. Compared with the patients in the control hospitals (n = 214), the patients in the intervention hospitals (n = 248) received significantly more days of enteral nutrition (6.7 v. 5.4 per 10 patient-days; p = 0.042), had a significantly shorter mean stay in hospital (25 v. 35 days; p = 0.003) and showed a trend toward reduced mortality (27% v. 37%; p = 0.058). The mean stay in the ICU did not differ between the control and intervention groups (10.9 v. 11.8 days; p = 0.7).
Interpretation: Implementation of evidence-based recommendations improved the provision of nutritional support and was associated with improved clinical outcomes.
Figures
Comment in
-
An evidence based algorithm for nutritional support accompanied by a multifaceted implementation strategy improved some outcomes in critically ill patients.Evid Based Nurs. 2004 Jul;7(3):89. doi: 10.1136/ebn.7.3.89. Evid Based Nurs. 2004. PMID: 15252917 No abstract available.
References
-
- Clifton GL, Robertson CS, Choi SC. Assessment of nutritional requirements of head-injured patients. J Neurosurg 1986;64:895-901. - PubMed
-
- Daley J, Khuri SF, Henderson W, Hur K, Gibbs JO, Barbour G, et al. Risk adjustment of the postoperative morbidity rate for the comparative assessment of the quality of surgical care: results of the National Veterans Affairs Surgical Risk Study. J Am Coll Surg 1997;185:328-40. - PubMed
-
- Dempsey DT, Mullen JL, Buzby GP. The link between nutritional status and clinical outcome: Can nutritional intervention modify it? Am J Clin Nutr 1988;47:352-6. - PubMed
-
- Heyland DK, MacDonald S, Keefe L, Drover JW. Total parenteral nutrition in the critically ill patient: a Meta-analysis. JAMA 1998;280:2013-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical