

Cost-effectiveness of stereotactic large-core needle biopsy for nonpalpable breast lesions compared to open-breast biopsy
- PMID: 14735181
- PMCID: PMC2409541
- DOI: 10.1038/sj.bjc.6601520
Cost-effectiveness of stereotactic large-core needle biopsy for nonpalpable breast lesions compared to open-breast biopsy
Abstract
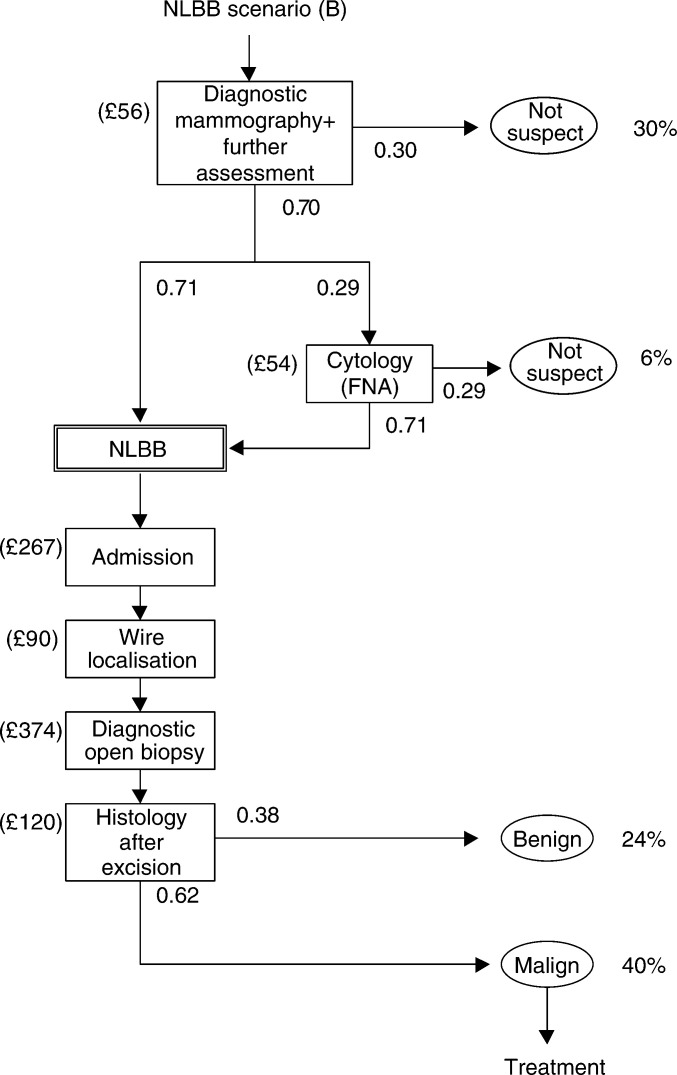
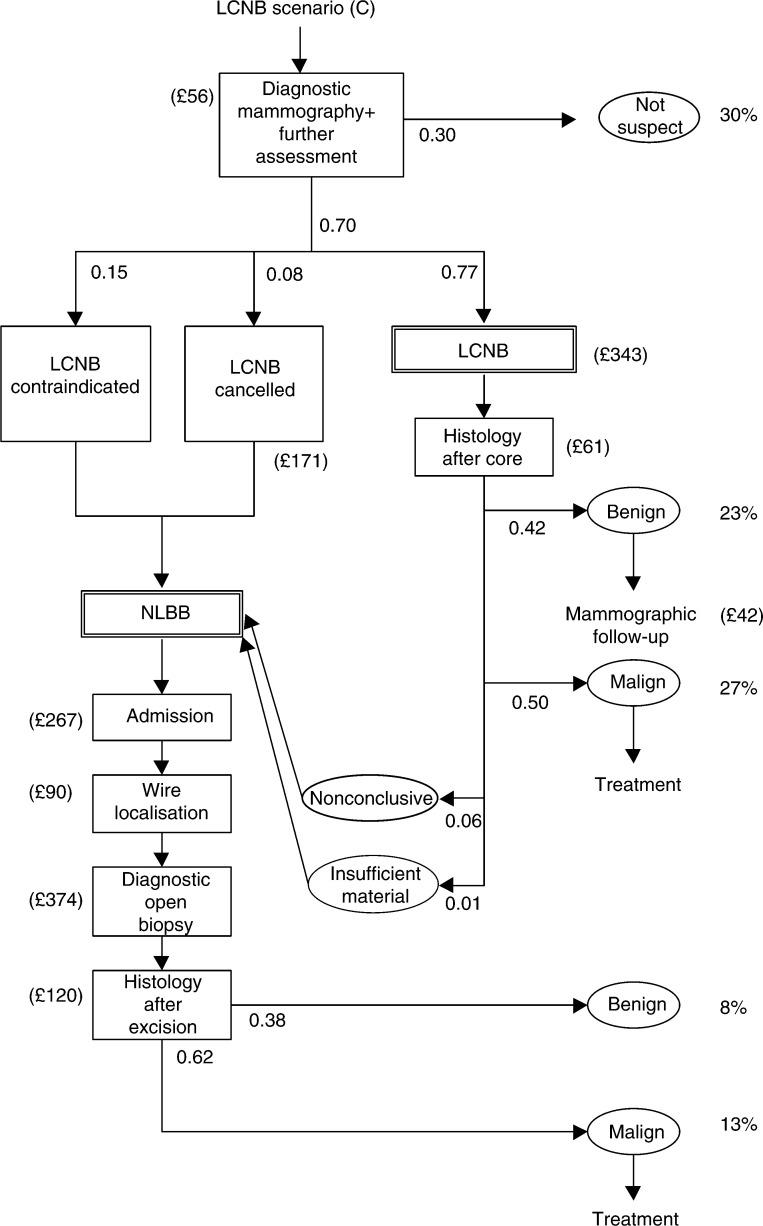
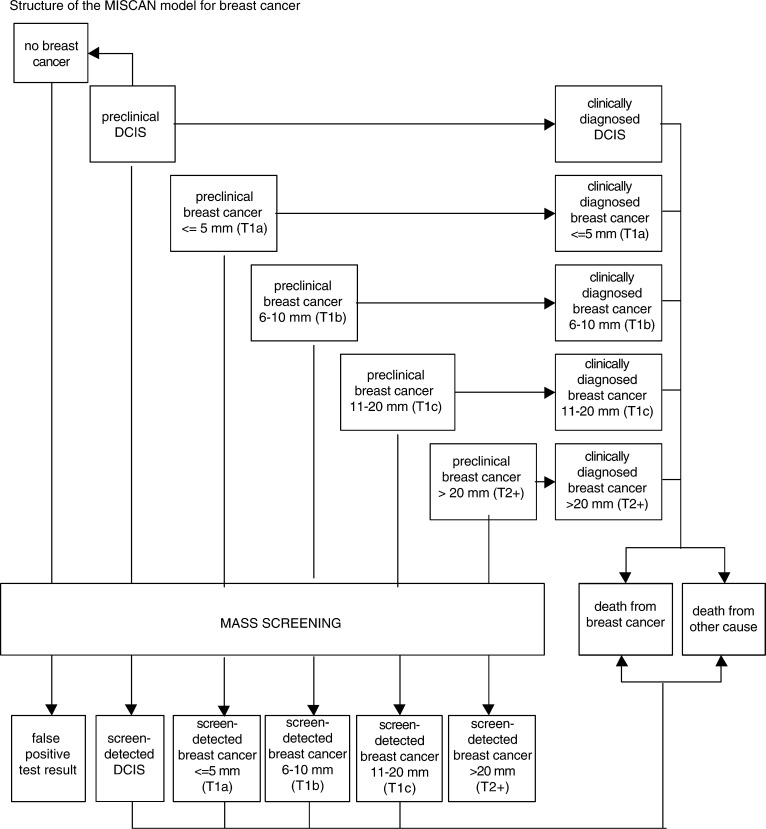
This paper demonstrates that the introduction of large-core needle biopsy (LCNB) replacing needle-localised breast biopsy (NLBB) for nonpalpable (screen-detected) breast lesions could result in substantial cost savings at the expense of a possible slight increase in breast cancer mortality. The cost-effectiveness of LCNB and NLBB was estimated using a microsimulation model. The sensitivity of LCNB (0.97) and resource use and costs of LCNB and NLBB were derived from a multicentre consecutive cohort study among 973 women who consented in getting LCNB and NLBB, if LCNB was negative. Sensitivity analyses were performed. Replacing NLBB with LCNB would result in approximately six more breast cancer deaths per year (in a target population of 2.1 million women), or in 1000 extra life-years lost from breast cancer (effect over 100 years). The total costs of management of breast cancer (3% discounted) are estimated at pound 4676 million with NLBB; introducing LCNB would save pound 13 million. The incremental cost-effectiveness ratio of continued NLBB vs LCNB would be pound 12 482 per additional life-year gained (3% discounted); incremental costs range from pound -21 687 (low threshold for breast biopsy) to pound 74 378 (high sensitivity of LCNB).
Figures
Similar articles
-
Diagnostic accuracy for different strategies of image-guided breast intervention in cases of nonpalpable breast lesions.Br J Cancer. 2004 Feb 9;90(3):595-600. doi: 10.1038/sj.bjc.6601559. Br J Cancer. 2004. PMID: 14760370 Free PMC article. Clinical Trial.
-
Efficiency of Core Biopsy for BI-RADS-5 Breast Lesions.Breast J. 2008 Sep-Oct;14(5):471-5. doi: 10.1111/j.1524-4741.2008.00624.x. Breast J. 2008. PMID: 18821933
-
Cost-effectiveness of stereotactic core needle biopsy: analysis by means of mammographic findings.Radiology. 1997 Mar;202(3):849-54. doi: 10.1148/radiology.202.3.9051045. Radiology. 1997. PMID: 9051045
-
Advances in the diagnosis and excision of breast cancer.Am Surg. 2003 Jan;69(1):11-4. Am Surg. 2003. PMID: 12575773 Review.
-
[Recent progress in the diagnosis of nonpalpable breast lesions].Nihon Geka Gakkai Zasshi. 1996 May;97(5):343-6. Nihon Geka Gakkai Zasshi. 1996. PMID: 8709935 Review. Japanese.
Cited by
-
The impact of healthcare costs in the last year of life and in all life years gained on the cost-effectiveness of cancer screening.Br J Cancer. 2009 Apr 21;100(8):1240-4. doi: 10.1038/sj.bjc.6605018. Br J Cancer. 2009. PMID: 19367281 Free PMC article.
-
Interpreting overdiagnosis estimates in population-based mammography screening.Epidemiol Rev. 2011;33(1):111-21. doi: 10.1093/epirev/mxr009. Epub 2011 Jun 27. Epidemiol Rev. 2011. PMID: 21709144 Free PMC article. Review.
-
Adjunctive self-hypnotic relaxation for outpatient medical procedures: a prospective randomized trial with women undergoing large core breast biopsy.Pain. 2006 Dec 15;126(1-3):155-64. doi: 10.1016/j.pain.2006.06.035. Epub 2006 Sep 7. Pain. 2006. PMID: 16959427 Free PMC article. Clinical Trial.
-
Evaluation of the predictive ability of ultrasound-based assessment of breast cancer using BI-RADS natural language reporting against commercial transcriptome-based tests.PLoS One. 2020 Jan 10;15(1):e0226634. doi: 10.1371/journal.pone.0226634. eCollection 2020. PLoS One. 2020. PMID: 31923222 Free PMC article.
-
Overdiagnosis and overtreatment of breast cancer: microsimulation modelling estimates based on observed screen and clinical data.Breast Cancer Res. 2006;8(1):202. doi: 10.1186/bcr1369. Epub 2005 Dec 21. Breast Cancer Res. 2006. PMID: 16524452 Free PMC article.
References
-
- BreastScreen Victoria (2000) BreastScreen Victoria 1998 Highlights
-
- Boer R, de Koning HJ, van Oortmarssen GJ, van der Maas PJ (1995) In search of the best upper age limit for breast cancer screening. Eur J Cancer 31A: 2040–2043 - PubMed
-
- Britton PD, Flower CD, Freeman AH, Sinnatamby R, Warren R, Goddard MJ, Wight DG, Bobrow L (1997) Changing to core biopsy in an NHS breast screening unit. Clin Radiol 52: 764–767 - PubMed
-
- Buijs-van der Woude T, Verkooijen HM, Pijnappel RM, Klinkenbijl JHG, Borel Rinkes IHM, Peeters PHM, Buskens E (2001) Cost comparison between stereotactic large-core-needle biopsy versus surgical excision biopsy in The Netherlands. Eur J Cancer 37: 1736–1745 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
