

Immune responses to glutamic acid decarboxylase and insulin in patients with gestational diabetes
- PMID: 14738462
- PMCID: PMC1808948
- DOI: 10.1111/j.1365-2249.2004.02355.x
Immune responses to glutamic acid decarboxylase and insulin in patients with gestational diabetes
Abstract
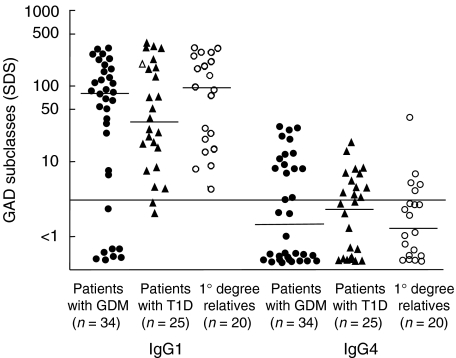
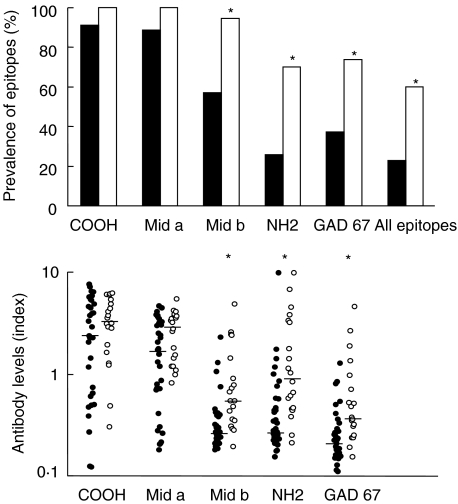
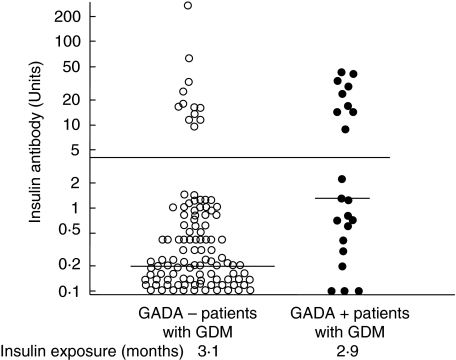
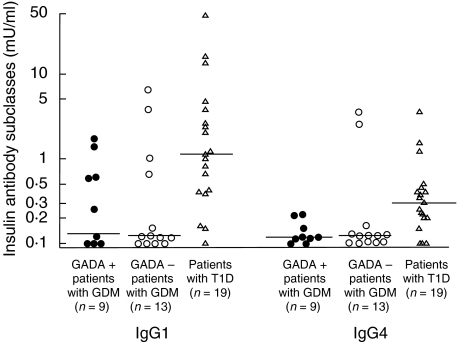
Pregnancy is a natural state of immunoprotection and tolerance. We studied subjects with gestational diabetes (GDM) to evaluate the influence of pregnancy on the humoral immune response to the autoantigen GAD and to injected insulin. Antibodies against glutamic acid decarboxylase (GADA) subclasses and epitope reactivity were determined in 34 GADA-positive pregnant patients with GDM, in 20 GADA-positive relatives of people with TID and in 25 GADA-positive patients with newly diagnosed TID. Partum levels of insulin antibodies (IA), IgG1- and IgG4-IA were measured in 131 women with GDM treated with human insulin from the time of diabetes diagnosis (including 22 with GADA) and were compared to 19 patients with TID after 3 months of insulin treatment. GADA titre and subclasses were similar among all groups. GADA in GDM patients bound fewer epitopes than GADA in relatives of patients with TID (all epitopes being present in 23%versus 65%, P < 0.01). In particular, antibodies to the minor GADA epitopes GAD6596-249, GAD651-100 and GAD67 were less frequent in patients with GDM compared to relatives (P < 0.01). Antibodies to insulin (IA) were found in 17% of patients with GDM. They were more frequent in GDM patients with GADA compared to GADA-negative patients (41%versus 12%, P < 0.005). IgG1 was the dominant insulin antibody subclass response in both patients with GDM and TID but levels of IgG1-IA and IgG4-IA were significantly lower in patients with GDM compared to patients with TID (P < 0.004). Antibody responses in women with gestational diabetes appear to be dampened and restricted, but without change in subclass usage.
Figures
Similar articles
-
The prevalence of GAD antibodies in Korean women with gestational diabetes mellitus and their clinical characteristics during and after pregnancy.Diabetes Metab Res Rev. 2009 May;25(4):329-34. doi: 10.1002/dmrr.963. Diabetes Metab Res Rev. 2009. PMID: 19405080
-
IgG4 subclass glutamic acid decarboxylase antibodies (GADA) are associated with a reduced risk of developing type 1 diabetes as well as increased C-peptide levels in GADA positive gestational diabetes.Clin Immunol. 2016 Jan;162:45-8. doi: 10.1016/j.clim.2015.11.001. Epub 2015 Nov 5. Clin Immunol. 2016. PMID: 26548838
-
Autoantibodies to GAD and IA-2 in Saudi Arabian diabetic patients.Diabet Med. 2005 Apr;22(4):448-52. doi: 10.1111/j.1464-5491.2005.01438.x. Diabet Med. 2005. PMID: 15787671
-
Anti-glutamic Acid Decarboxylase Antibody-Positive Gestational Diabetes Mellitus with Autoimmune Type 1 Diabetes Mellitus in the Early Postpartum Period: A Case Report and Literature Review.Tohoku J Exp Med. 2023 Apr 8;259(4):327-333. doi: 10.1620/tjem.2023.J013. Epub 2023 Feb 23. Tohoku J Exp Med. 2023. PMID: 36823183 Review.
-
Glutamic Acid Decarboxylase Autoantibody-negative Slowly Progressive Type 1 Diabetes Mellitus: A Case Report and Literature Review.Intern Med. 2018 Dec 15;57(24):3581-3587. doi: 10.2169/internalmedicine.1008-18. Epub 2018 Aug 10. Intern Med. 2018. PMID: 30101912 Free PMC article. Review.
References
-
- Raghupathy R, Makhseed M, Azizieh F, Hassan N, Al-Azemi M, Al-Shamali E. Maternal Th1- and Th2-type reactivity to placental antigens in normal human pregnancy and unexplained recurrent spontaneous abortion. Cell Immunol. 1999;196:122–30. - PubMed
-
- Ostensen M. Sex hormones and pregnancy in rheumatoid arthritis and systemic lupus erythematodes. Ann NY Acad Sci. 1999;876:131–43. - PubMed
-
- Füchtenbusch M, Ferber K, Standl E, Ziegler AG. Prediction of type I diabetes postpartum in patients with gestational diabetes mellitus by combined islet cell autoantibody screening. A prospective multicenter study. Diabetes. 1997;46:1459–67. - PubMed
-
- Dittler J, Seidel D, Schenker M, Ziegler A-G. GADAIA2-combi determination as first-line screening for improved prediction of type 1 diabetes in relatives. Diabetes. 1998;47:592–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
