

Obesity decreases perioperative tissue oxygenation
- PMID: 14739800
- PMCID: PMC1395476
- DOI: 10.1097/00000542-200402000-00015
Obesity decreases perioperative tissue oxygenation
Abstract
Background: Obesity is an important risk factor for surgical site infections. The incidence of surgical wound infections is directly related to tissue perfusion and oxygenation. Fat tissue mass expands without a concomitant increase in blood flow per cell, which might result in a relative hypoperfusion with decreased tissue oxygenation. Consequently, the authors tested the hypotheses that perioperative tissue oxygen tension is reduced in obese surgical patients. Furthermore, they compared the effect of supplemental oxygen administration on tissue oxygenation in obese and nonobese patients.
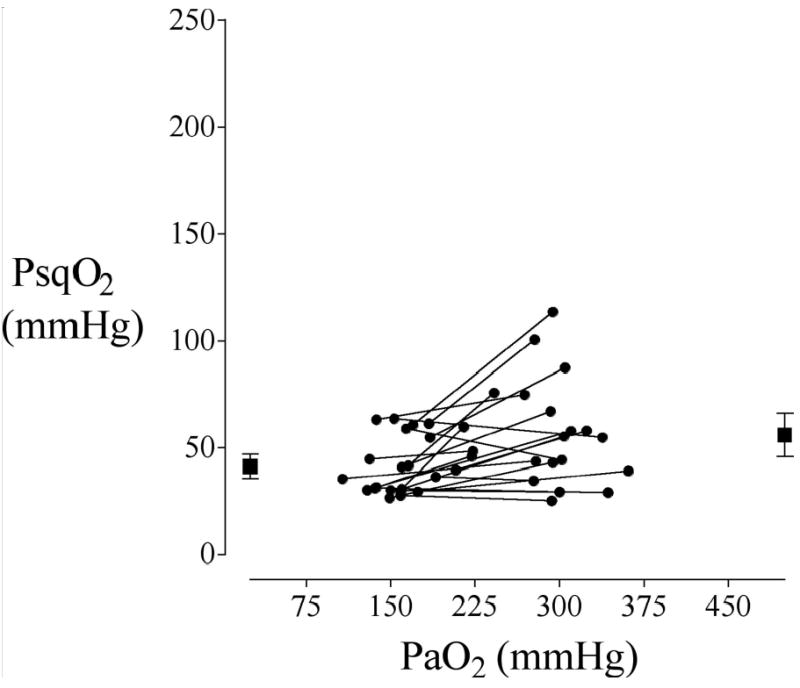
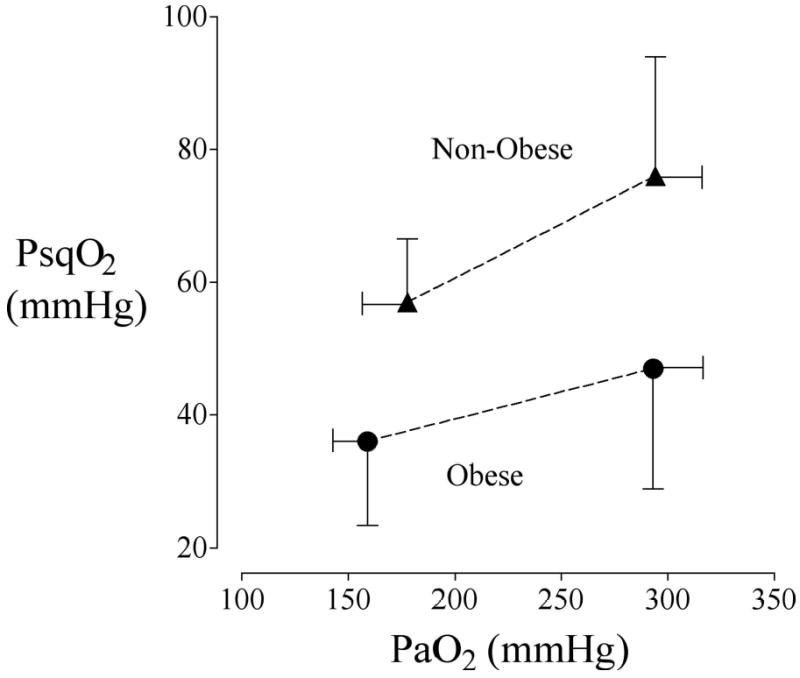
Methods: Forty-six patients undergoing major abdominal surgery were assigned to one of two groups according to their body mass index: body mass index less than 30 kg/m2 (nonobese) or 30 kg/m2 or greater (obese). Intraoperative oxygen administration was adjusted to arterial oxygen tensions of approximately 150 mmHg and approximately 300 mmHg in random order. Anesthesia technique and perioperative fluid management were standardized. Subcutaneous tissue oxygen tension was measured with a polarographic electrode positioned within a subcutaneous tonometer in the lateral upper arm during surgery, in the recovery room, and on the first postoperative day. Postoperative tissue oxygen was also measured adjacent to the wound. Data were compared with unpaired two-tailed t tests and Wilcoxon rank sum test; P < 0.05 was considered statistically significant.
Results: Intraoperative subcutaneous tissue oxygen tension was significantly less in the obese patients at baseline (36 vs. 57 mmHg; P = 0.002) and with supplemental oxygen administration (47 vs. 76 mmHg; P = 0.014). Immediate postoperative tissue oxygen tension was also significantly less in subcutaneous tissue of the upper arm (43 vs. 54 mmHg; P = 0.011) as well as near the incision (42 vs. 62 mmHg; P = 0.012) in obese patients. In contrast, tissue oxygen tension was comparable in each group on the first postoperative morning.
Conclusion: Wound and tissue hypoxia were common in obese patients in the perioperative period and most pronounced during surgery. Even with supplemental oxygen tissue, oxygen tension in obese patients was reduced to levels that are associated with a substantial increase in infection risk.
Figures

References
-
- Babior BM. Oxygen-dependent microbial killing by phagocytes. N Engl J Med. 1978;298:659–68. - PubMed
-
- Hopf HW, Hunt TK, West JM, Blomquist P, Goodson WH, 3rd, Jensen JA, Jonsson K, Paty PB, Rabkin JM, Upton RA, von Smitten K, Whitney JD. Wound tissue oxygen tension predicts the risk of wound infection in surgical patients. Arch Surg 1997; 132: 997–1004; discussion 1005 - PubMed
-
- Gottrup F. Physiology and measurement of tissue perfusion. Ann Chir Gynaecol. 1994;83:183–9. - PubMed
-
- Van Esbroeck G, Gys T, Hubens A. Evaluation of tissue oximetry in perioperative monitoring of colorectal surgery. Br J Surg. 1992;79:584–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
