

Clinical efficacy of antiretroviral combination therapy based on protease inhibitors or non-nucleoside analogue reverse transcriptase inhibitors: indirect comparison of controlled trials
- PMID: 14742351
- PMCID: PMC324449
- DOI: 10.1136/bmj.37995.435787.A6
Clinical efficacy of antiretroviral combination therapy based on protease inhibitors or non-nucleoside analogue reverse transcriptase inhibitors: indirect comparison of controlled trials
Abstract
Objective: To compare the clinical efficacy of triple antiretroviral regimens based on protease inhibitors and non-nucleoside analogue reverse transcriptase inhibitors (NNRTIs) in adults positive for antibodies to HIV-1.
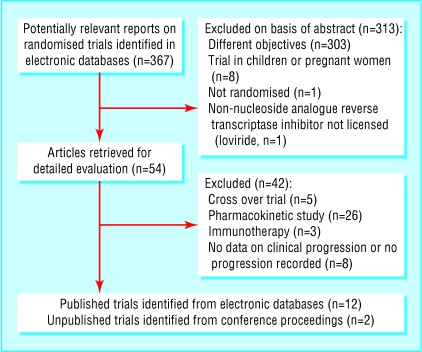
Design: Systematic review and meta-analysis using indirect comparisons of clinical trials comparing three drug regimens based on two nucleoside reverse transcriptase inhibitors (NRTIs) and either a protease inhibitor or an NNRTI with two drug regimens (two NRTIs). Participants had no previous exposure to protease inhibitors or NNRTIs.
Data sources: Medline, the Cochrane controlled trials register, Aidstrials, Aidsdrugs, conference proceedings, and trial registers.
Main outcome measure: Progression to AIDS or death.
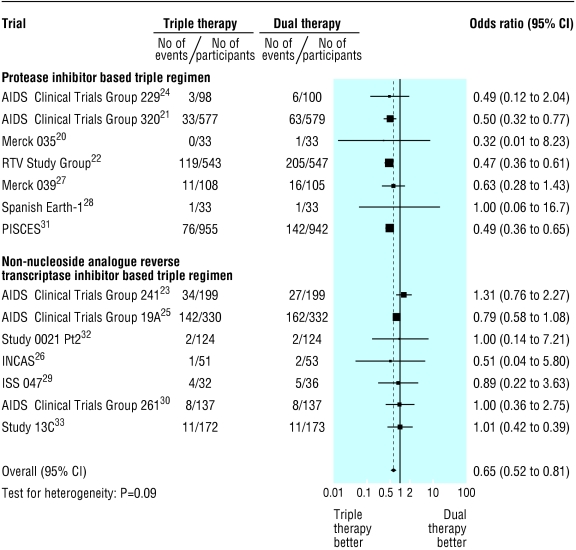
Results: 14 trials, totalling 6785 patients, were identified. Most patients had been exposed to an NRTI and had advanced immunodeficiency at baseline; 1096 progressed to AIDS or died. Seven trials assessed protease inhibitors based triple regimens and seven assessed NNRTI based triple regimens (nevirapine or delavirdine). Triple therapy was more effective than dual therapy. The effect was pronounced for protease inhibitor based regimens (odds ratio 0.49, 95% confidence interval 0.41 to 0.58) but non-significant for NNRTI based regimens (0.90, 0.71 to 1.15). Indirect comparison of the two regimens gave an odds ratio of 0.54 (0.49 to 0.73) in favour of protease inhibitor based treatments. Increases in CD4 cell counts were smaller and suppression of viral replication less with NNRTI based regimens.
Conclusions: Indirect evidence shows that protease inhibitor based triple regimens are superior to regimens based on the NNRTIs nevirapine and delavirdine in patients with advanced immunodeficiency who have been exposed to NRTIs. Large trials with clinical end points are required.
Figures

Comment in
-
Indirect comparisons: a novel approach to assessing the effect of anti-HIV drugs.BMJ. 2004 Jan 31;328(7434):253. doi: 10.1136/bmj.328.7434.253. BMJ. 2004. PMID: 14751897 Free PMC article. No abstract available.
References
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, Gargalianos P, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet 1998;352: 1725-30. - PubMed
-
- Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998;338: 853-60. - PubMed
-
- Staszewski S, Morales-Ramirez J, Tashima KT, Rachlis A, Skiest D, Stanford J, et al. Efavirenz plus zidovudine and lamivudine, efavirenz plus indinavir, and indinavir plus zidovudine and lamivudine in the treatment of HIV-1 infection in adults. Study 006 Team. N Engl J Med 1999;341: 1865-73. - PubMed
-
- Walmsley S, Bernstein B, King M, Arribas J, Beall G, Ruane P, et al. Lopinavir-ritonavir versus nelfinavir for the initial treatment of HIV infection. N Engl J Med 2002;346: 2039-46. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials