

Randomised controlled trial of labouring in water compared with standard of augmentation for management of dystocia in first stage of labour
- PMID: 14744822
- PMCID: PMC338094
- DOI: 10.1136/bmj.37963.606412.EE
Randomised controlled trial of labouring in water compared with standard of augmentation for management of dystocia in first stage of labour
Abstract
Objectives: To evaluate the impact of labouring in water during first stage of labour on rates of epidural analgesia and operative delivery in nulliparous women with dystocia.
Design: Randomised controlled trial.
Setting: University teaching hospital in southern England.
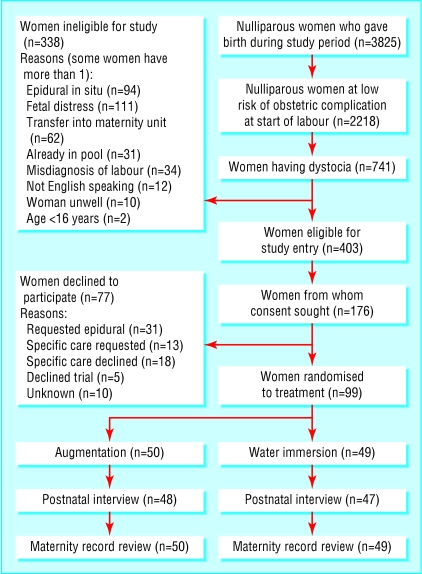
Participants: 99 nulliparous women with dystocia (cervical dilation rate < 1 cm/hour in active labour) at low risk of complications. Interventions Immersion in water in birth pool or standard augmentation for dystocia (amniotomy and intravenous oxytocin).
Main outcome measures: Primary: epidural analgesia and operative delivery rates. Secondary: augmentation rates with amniotomy and oxytocin, length of labour, maternal and neonatal morbidity including infections, maternal pain score, and maternal satisfaction with care.
Results: Women randomised to immersion in water had a lower rate of epidural analgesia than women allocated to augmentation (47% v 66%, relative risk 0.71 (95% confidence interval 0.49 to 1.01), number needed to treat for benefit (NNT) 5). They showed no difference in rates of operative delivery (49% v 50%, 0.98 (0.65 to 1.47), NNT 98), but significantly fewer received augmentation (71% v 96%, 0.74 (0.59 to 0.88), NNT 4) or any form of obstetric intervention (amniotomy, oxytocin, epidural, or operative delivery) (80% v 98%, 0.81 (0.67 to 0.92), NNT 5). More neonates of women in the water group were admitted to the neonatal unit (6 v 0, P = 0.013), but there was no difference in Apgar score, infection rates, or umbilical cord pH.
Conclusions: Labouring in water under midwifery care may be an option for slow progress in labour, reducing the need for obstetric intervention, and offering an alternative pain management strategy.
Comment in
-
Labouring in water: findings do not fully support conclusions.BMJ. 2004 Mar 27;328(7442):767-8; author reply 768. doi: 10.1136/bmj.328.7442.767-c. BMJ. 2004. PMID: 15044299 Free PMC article. No abstract available.
-
Labouring in water: method is unclear.BMJ. 2004 Mar 27;328(7442):767; author reply 768. doi: 10.1136/bmj.328.7442.767-b. BMJ. 2004. PMID: 15044300 Free PMC article. No abstract available.
-
Labouring in water: cover wrongly said study was about giving birth in water.BMJ. 2004 Mar 27;328(7442):768; discussion 768. doi: 10.1136/bmj.328.7442.768-a. BMJ. 2004. PMID: 15044302 Free PMC article. No abstract available.
References
-
- Department of Health. NHS maternity statistics, England 1989/90 to 1994/95. Statistical Bulletin No 28. London: Stationery Office, 1997: 1-16.
-
- Impey L, Boylan P. Active management of labour revisited. Br J Obstet Gynaecol 1999;106: 183-7. - PubMed
-
- Cammu H, Van Eeckhout E. A randomised controlled trial of early versus delayed use of amniotomy and oxytocin infusion in nulliparous labour. Br J Obstet Gynaecol 1996;103: 313-8. - PubMed
-
- Sadler LC, Davison T, McCowen LME. A randomised controlled trial and meta analysis of active management of labour. Br J Obstet Gynaecol 2000;107: 909-15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical