

Adult living donor liver transplantation for patients with hepatocellular carcinoma: extending UNOS priority criteria
- PMID: 14745320
- PMCID: PMC1356205
- DOI: 10.1097/01.sla.0000109022.32391.eb
Adult living donor liver transplantation for patients with hepatocellular carcinoma: extending UNOS priority criteria
Abstract
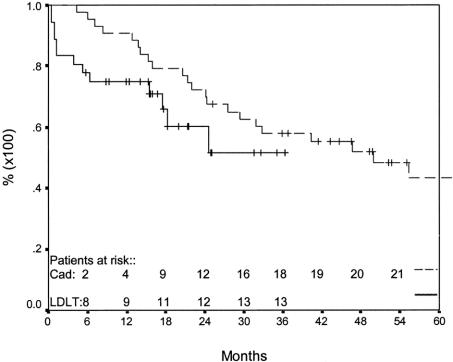
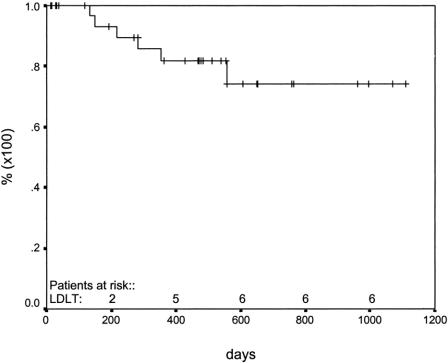
For patients with hepatocellular carcinoma (HCC) in particular, living donor liver transplant (LDLT) improves access to transplant. We report our results in 36 patients with HCC who underwent LDLT with a median follow-up >1 year. METHODS Underlying diagnoses included: hepatitis C (24), hepatitis B (9), cryptogenic cirrhosis (1), hemochromatosis (1), and primary biliary cirrhosis (1). Patients with tumors >or= 5 cm received IV doxorubicin intraoperatively and 6 cycles of doxorubicin at 3-week intervals. Patients were followed with CT scan and alpha-fetoprotein levels every 3 months for 2 years posttransplant. Mean waiting time, pretransplant treatment, tumor variables, and survival were analyzed. Univariate and multivariate analysis were done to analyze tumor variables; Kaplan-Meier and log rank were used to compare survivals. P < 0.05 was considered significant. RESULTS Mean wait for LDLT was 62 days, compared with 459 days in 50 patients with HCC transplanted with cadaveric organs during the same time period (P = 0.0001). At median follow-up of 450 days, there have been 10 deaths due to non-tumor-related causes and 3 deaths from recurrence; recurrence has also been observed in 3 other patients. On univariate and multivariate analysis, bilobar distribution was the only significant tumor variable (P = 0.03, log rank = 0.02). Fifty-three percent of patients exceeded UNOS priority criteria. One- and two-year patient survivals were 75% and 60%, respectively. Freedom from recurrence at 365 and 730 days was 82% and 74%, respectively. Overall and in patients with HCC > 5 cm (n = 12), there were no statistically significant differences in survival or in freedom from recurrence between recipients of living donor and cadaveric grafts. CONCLUSION Although one third of patients had tumors > 5 cm, the incidence of recurrence as well as patient survival and freedom from recurrence are comparable to results after cadaveric transplant. LDLT allows timely transplantation in patients with early or with large HCC.
Figures

Comment on
-
Challenging choices: liver transplantation for hepatocellular carcinoma.Ann Surg. 2004 Feb;239(2):160-1. doi: 10.1097/01.sla.0000109169.72607.50. Ann Surg. 2004. PMID: 14745322 Free PMC article. No abstract available.
References
-
- Okuda K. Hepatocellular carcinoma: recent progress. Hepatology. 1992;15:948–963. - PubMed
-
- Calvet X, Bruix J, Bru C, et al. Natural history of hepatocellular carcinoma in Spain. Five year's experience in 249 cases. J Hepatol. 1990;16:6–72. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;14:728–729. - PubMed
-
- Barbara L, Benzi G, Gaiani S, et al. Natural history of small untreated hepatocellular carcinoma: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology. 1992;16:132–137. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
