

Basic advances and new avenues in therapy of spinal cord injury
- PMID: 14746521
- PMCID: PMC4164205
- DOI: 10.1146/annurev.med.55.091902.104338
Basic advances and new avenues in therapy of spinal cord injury
Abstract
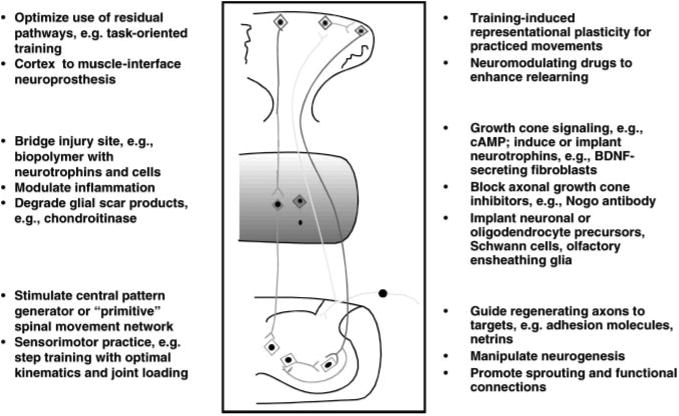
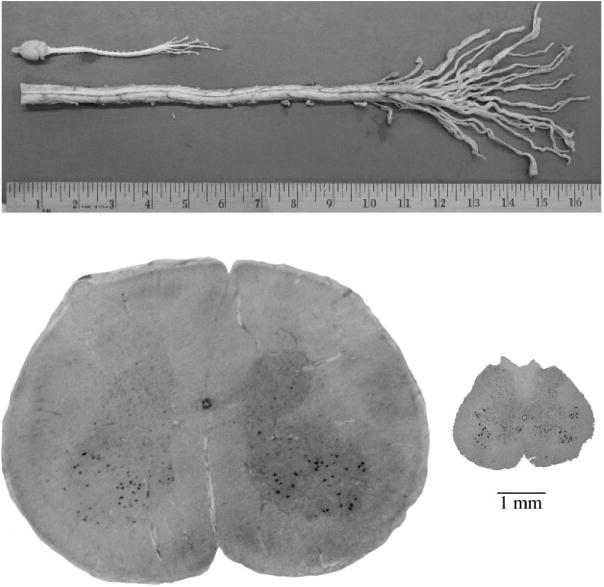
The prospects for successful clinical trials of neuroprotective and neurorestorative interventions for patients with acute and chronic myelopathies depend on preclinical animal models of injury and repair that reflect the human condition. Remarkable progress continues in the attempt to promote connections between the brain and the sensory and motor neurons below a spinal cord lesion. Recent experiments demonstrate the potential for biological therapies to regenerate or remyelinate axons and to incorporate new neural cells into the milieu of a traumatic spinal cord injury. The computational flexibility and plasticity of the sensorimotor systems of the brain, spinal cord, and motor unit make functional use of new circuitry feasible in patients. To incorporate residual and new pathways, neural repair strategies must be coupled to rehabilitation therapies that drive activity-dependent plasticity for walking, for reaching and grasping, and for bowel and bladder control. Prevention of pain and dysautonomia are also clinical targets. Research aims to define the temporal windows of opportunity for interventions, test the safety and efficacy of delivery systems of agents and cells, and provide a better understanding of the cascades of gene expression and cell interactions both acutely and chronically after injury. These bench-to-bedside studies are defining the neurobiology of spinal cord injury rehabilitation.
Figures
References
-
- Raineteau O, Schwab M. Plasticity of motor systems after incomplete spinal cord injury. Nat Rev Neurosci. 2001;2:263–73. - PubMed
-
- Dobkin BH. The Clinical Science of Neurologic Rehabilitation. New York: Oxford Univ Press; 2003.
-
- Maniar H, Sundt T, Prasad S, et al. Delayed paraplegia after thoracic and thoracoabdominal aneurysm repair: a continuing risk. Ann Thorac Surg. 2003;75:113–20. - PubMed
-
- Kwon B, Oxland T, Tetzlaff W. Animal models used in spinal cord regeneration research. Spine. 2002;27:1504–10. - PubMed
-
- Inman D, Guth L, Steward O. Genetic influences on secondary degeneration and wound healing following spinal cord injury in various strains of mice. J Comp Neurol. 2002;451:225–35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
