

Agreement between preoperative core needle biopsy and postoperative invasive breast cancer histopathology is not dependent on the amount of clinical material obtained
- PMID: 14747449
- PMCID: PMC1770204
- DOI: 10.1136/jcp.2003.12914
Agreement between preoperative core needle biopsy and postoperative invasive breast cancer histopathology is not dependent on the amount of clinical material obtained
Abstract
Aims: To establish the relation between the amount of breast core needle biopsy (CNB) material examined and agreement between preoperative and postoperative histopathology parameters in invasive breast cancer.
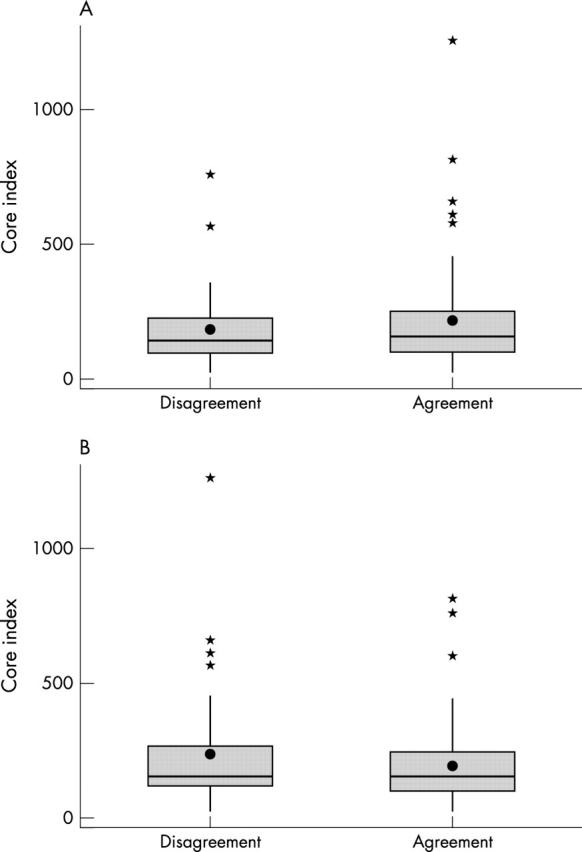
Methods: The CNB and surgical specimen histopathology reports of 113 patients with invasive breast carcinoma were reviewed and the total amount of CNB material examined for each case was determined. Agreement was calculated for tumour type, grade, mitoses, nuclear pleomorphism, and tubule formation. Associations between the amount of CNB material and histopathology agreement before and after surgery were explored using binary logistic regression.
Results: Tumour type and grade agreed in 65.4% and 61.6% of cases, respectively. The components used to calculate grade--nuclear pleomorphism (57.4%), mitoses (59.4%), and tubule formation (55.6%)--agreed slightly less frequently. The proportion of cases with preoperative and postoperative assessments that agreed did not depend on the number of cores collected or the total amount of material examined.
Conclusion: Neither tumour type and grade, nor the individual components used to calculate grade agreed consistently between the CNB and surgical specimen. The number of cores collected and the total amount of material reviewed by the pathologist does not influence the likelihood of agreement between preoperative and postoperative histopathology reports.
Figures
References
-
- Pinder SE, Elston CW, Ellis IO. The role of pre-operative diagnosis in breast cancer. Histopathology 1996;28:563–6. - PubMed
-
- Non-operative Diagnosis Subgroup of the National Coordinating Group for Breast Screening Pathology. Guidelines for non-operative diagnostic procedures and reporting in breast cancer screening. Sheffield: NHS Cancer Screening Programmes 2001 (NHS Publication No. 50, ISBN 1 871997 44 5).
-
- Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long term follow-up Histopathology 1991;19:403–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical