

The human, societal, and scientific legacy of cholera
- PMID: 14755327
- PMCID: PMC324550
- DOI: 10.1172/JCI20982
The human, societal, and scientific legacy of cholera
Abstract
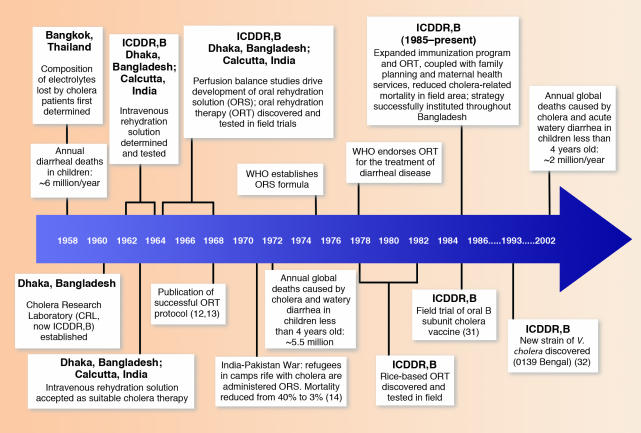
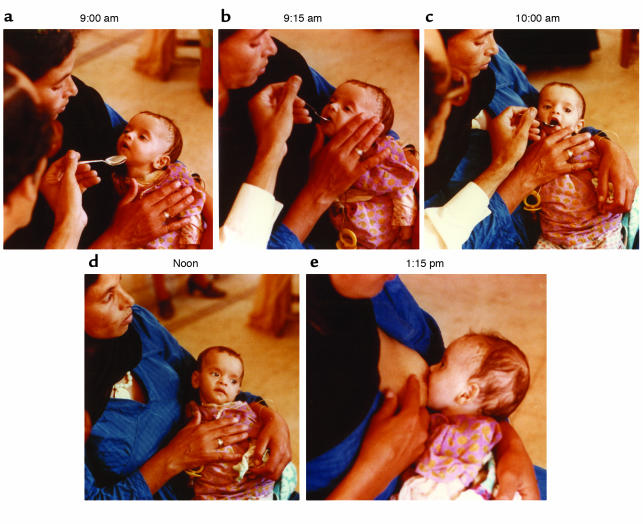
The recent history of research on cholera illustrates the importance of establishing research and care facilities equipped with advanced technologies at locations where specific health problems exist. It is in such settings, where scientific research is often considered difficult due to poverty and the lack of essential infrastructure, that investigators from many countries are able to make important advances. On this, the 25th anniversary of the founding of the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), this article seeks to recount the Centre's demonstration of how high-quality research on important global health issues, including cholera, can be accomplished in conditions that may be considered by many as unsuitable for scientific research.
Figures
References
-
- Rohde, J.E., and Northrup, R.S. 1976. Taking science where the diarrhoea is. In Acute diarrhoea in childhood. CIBA Foundation Symposium 42. Elsevier. Amsterdam, The Netherlands. 339–358. - PubMed
-
- Carpenter CCJ. Treatment of cholera — tradition and authority versus science, reason and humanity. Johns Hopkins Med. J. 1976;139:153–162. - PubMed
-
- Evenson RE, Gollin D. Assessing the impact of the green revolution, 1960 to 2000. Science. 2003;300:758–762. - PubMed
-
- Colwell RR. Global climate and infectious disease: the cholera paradigm. Science. 1996;274:2025–2031. - PubMed
