

Autoreactive T cell responses show proinflammatory polarization in diabetes but a regulatory phenotype in health
- PMID: 14755342
- PMCID: PMC324541
- DOI: 10.1172/JCI19585
Autoreactive T cell responses show proinflammatory polarization in diabetes but a regulatory phenotype in health
Abstract
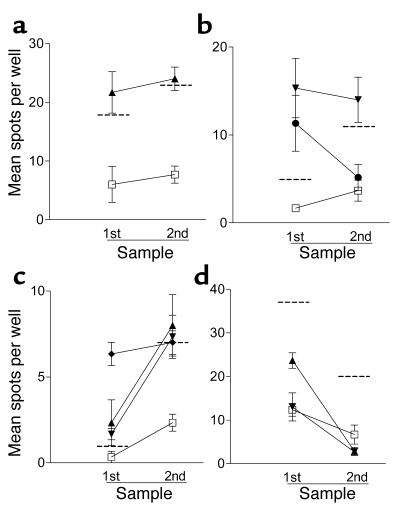
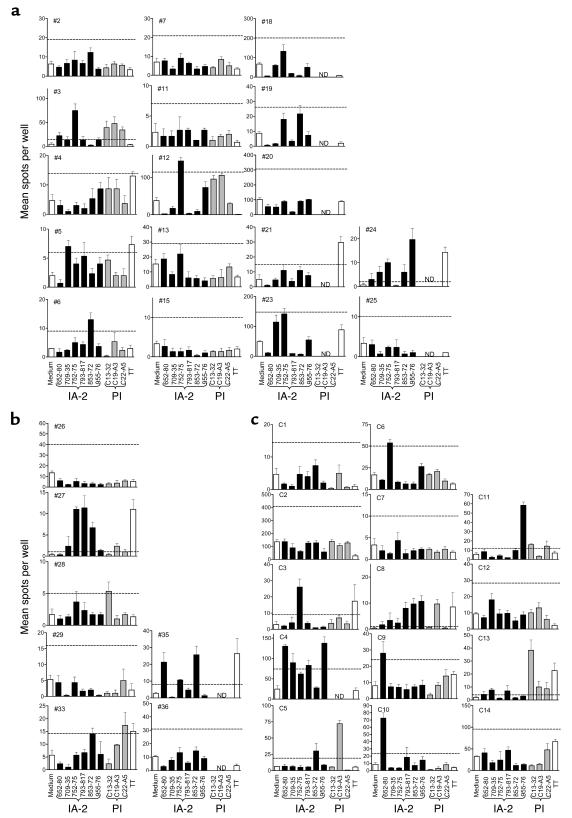
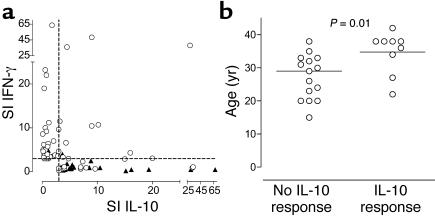
According to the quality of response they mediate, autoreactive T cells recognizing islet beta cell peptides could represent both disease effectors in the development of type 1 diabetes (T1DM) and directors of tolerance in nondiabetic individuals or those undergoing preventative immunotherapy. A combination of the rarity of these cells, inadequate technology, and poorly defined epitopes, however, has hampered examination of this paradigm. We have identified a panel of naturally processed islet epitopes by direct elution from APCs bearing HLA-DR4. Employing these epitopes in a sensitive, novel cytokine enzyme-linked immunosorbent spot assay, we show that the quality of autoreactive T cells in patients with T1DM exhibits extreme polarization toward a proinflammatory Th1 phenotype. Furthermore, we demonstrate that rather than being unresponsive, the majority of nondiabetic, HLA-matched control subjects also manifest a response against islet peptides, but one that shows extreme T regulatory cell (Treg, IL-10-secreting) bias. We conclude that development of T1DM depends on the balance of autoreactive Th1 and Treg cells, which may be open to favorable manipulation by immune intervention.
Figures
Comment in
-
Achieving antigen-specific immune regulation.J Clin Invest. 2004 Feb;113(3):346-9. doi: 10.1172/JCI20963. J Clin Invest. 2004. PMID: 14755329 Free PMC article. Review.
References
-
- Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet. 2001;358:221–229. - PubMed
-
- Raz I, et al. Beta-cell function in new-onset type 1 diabetes and immunomodulation with a heat-shock protein peptide (DiaPep277): a randomised, double-blind, phase II trial. Lancet. 2001;358:1749–1753. - PubMed
-
- Schatz DA, Bingley PJ. Update on major trials for the prevention of type 1 diabetes mellitus: the American Diabetes Prevention Trial (DPT-1) and the European Nicotinamide Diabetes Intervention Trial (ENDIT) J. Pediatr. Endocrinol. Metab. 2001;14(Suppl 1):619–622. - PubMed
-
- Diabetes Prevention Trial—Type 1 Diabetes Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N. Engl. J. Med. 2002;346:1685–1691. - PubMed
-
- Herold KC, et al. Anti-CD3 monoclonal antibody in new-onset type 1 diabetes mellitus. N. Engl. J. Med. 2002;346:1692–1698. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
