

Increasing prevalence of vancomycin-resistant Enterococcus faecium, expanded-spectrum cephalosporin-resistant Klebsiella pneumoniae, and imipenem-resistant Pseudomonas aeruginosa in Korea: KONSAR study in 2001
- PMID: 14966334
- PMCID: PMC2822269
- DOI: 10.3346/jkms.2004.19.1.8
Increasing prevalence of vancomycin-resistant Enterococcus faecium, expanded-spectrum cephalosporin-resistant Klebsiella pneumoniae, and imipenem-resistant Pseudomonas aeruginosa in Korea: KONSAR study in 2001
Abstract
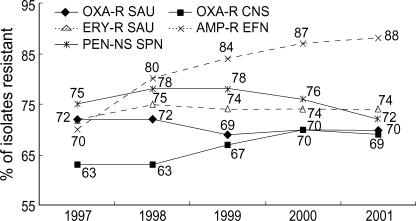
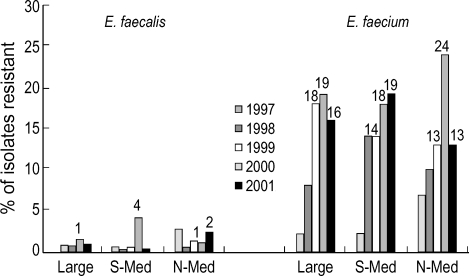
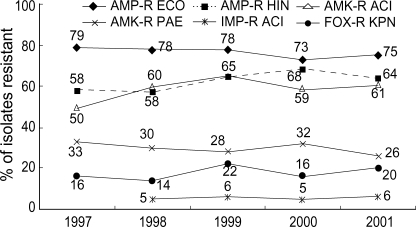
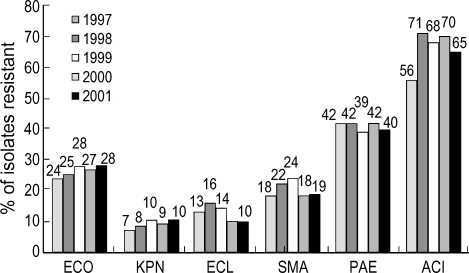
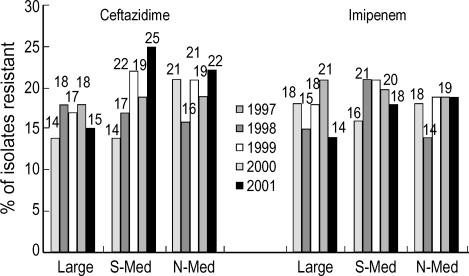
The 5th year KONSAR surveillance in 2001 was based on routine test data at 30 participating hospitals. It was of particular interest to find a trend in the resistances of enterococci to vancomycin, of Enterobacteriaceae to the 3rd generation cephalosporin and fluoroquinolone, and of Pseudomonas aeruginosa and acinetobacters to carbapenem. Resistance rates of Gram-positive cocci were: 70% of Staphylococcus aureus to oxacillin; 88% and 16% of Enterococcus faecium to ampicillin and vancomycin, respectively. Seventy-two percent of pneumococci were nonsusceptible to penicillin. The resistance rates of Enterobacteriaceae were: Escherichia coli, 28% to fluoroquinolone; Klebsiella pneumoniae, 27% to ceftazidime, and 20% to cefoxitin; and Enterobacter cloacae, > or =40% to cefotaxime and ceftazidime. The resistance rates of P. aeruginosa were 21% to ceftazidime, 17% to imipenem, and those of the acinetobacters were > or =61% to ceftazidime, aminoglycosides, fluoroquinolone and cotrimoxazole. Thirty-five percent of non-typhoidal salmonellae were ampicillin resistant, and 66% of Haemophilus influenzae were beta-lactamase producers. Notable changes over the 1997-2001 period were: increases in vancomycin-resistant E. faecium, and amikacin- and fluoroquinolone-resistant acinetobacters. With the increasing prevalence of resistant bacteria, nationwide surveillance has become more important for optimal patient management, for the control of nosocomial infection, and for the conservation of the newer antimicrobial agents.
Figures
References
-
- Hunter PA, Reeves DS. The current status of surveillance of resistance to antimicrobial agents: report on a meeting. J Antimicrob Chemother. 2002;49:17–23. - PubMed
-
- Cosgrove SE, Carmeli Y. The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis. 2003;36:1433–1437. - PubMed
-
- Voss A, Milatovic D, Wallrauch-Schwarz C, Rosdahl VT, Braveny I. Methicillin-resistant Staphylococcus aureus in Europe. Eur J Clin Microbiol Infect Dis. 1994;13:50–55. - PubMed
-
- Sorberg M, Farra A, Ransjo U, Gardlund B, Rylander M, Settergren B, Kalin M, Kronvall G. Different trends in antibiotic resistance rates at a university teaching hospital. Clin Microbiol Infect. 2003;9:388–396. - PubMed
-
- Morris AK, Masterton RG. Antibiotic resistance surveillance: action for international studies. J Antimicrob Chemother. 2002;49:7–10. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
