

Endovascular treatment of intracranial wide-necked aneurysms using three-dimensional coils: predictors of immediate anatomic and clinical results
- PMID: 14970036
- PMCID: PMC7974599
Endovascular treatment of intracranial wide-necked aneurysms using three-dimensional coils: predictors of immediate anatomic and clinical results
Abstract
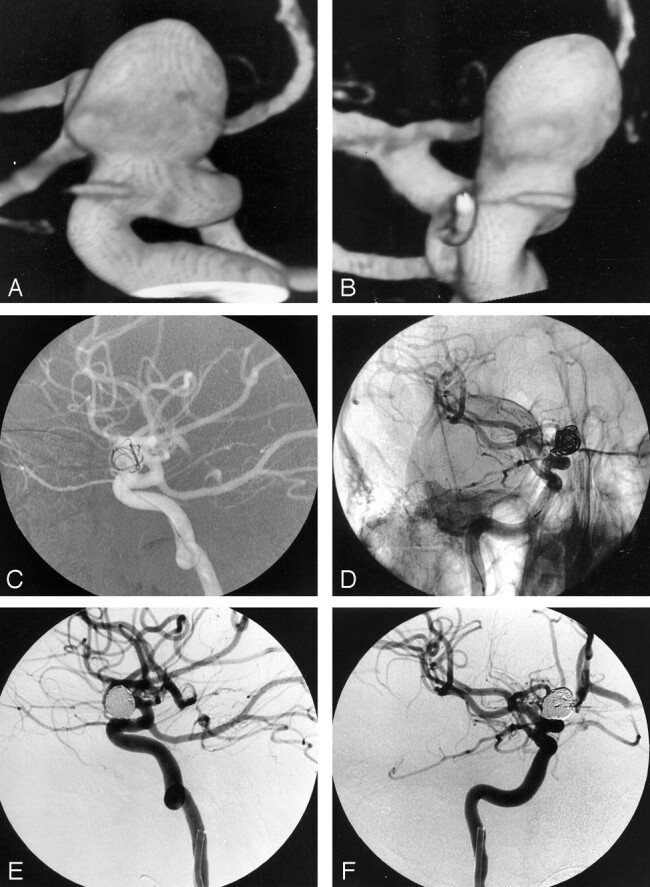
Background and purpose: Aneurysms with a wide neck constitute a persistent challenge for endovascular therapy with coils. Our purpose was to evaluate the immediate anatomic and clinical results of treating intracranial wide-necked aneurysms by using three-dimensional (3D) coils.
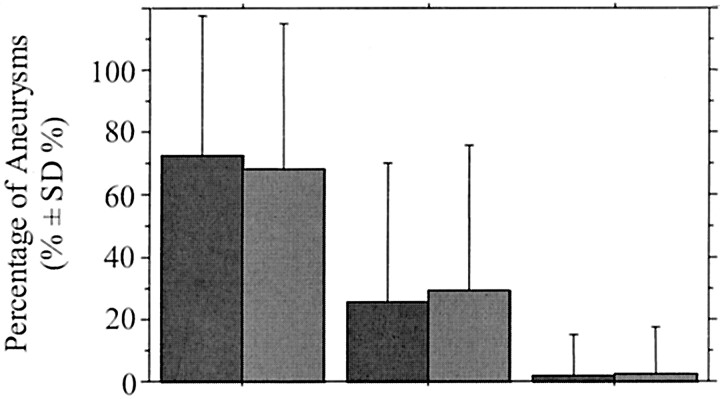
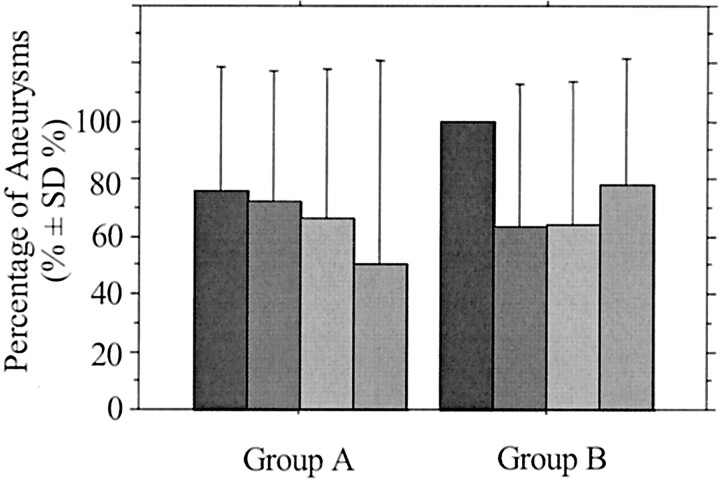
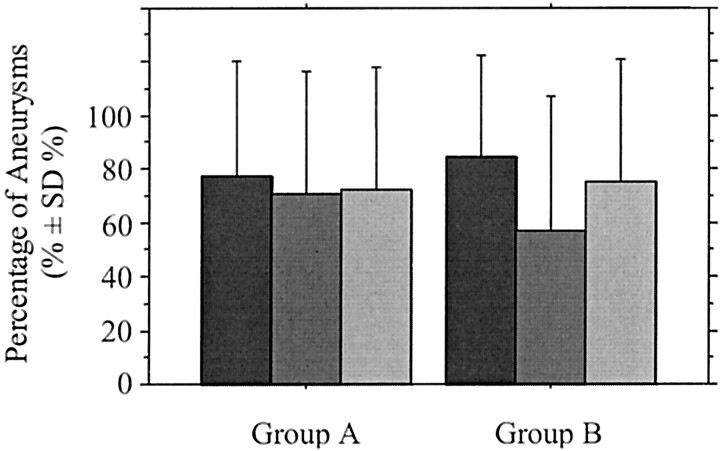
Methods: During a 2-year period, 160 aneurysms (116 with a neck < or = 4 mm, group A; 44 with a neck > 4 mm, group B) in 157 patients in eight participating centers were consecutively treated. The procedure consisted first of framing the aneurysm with one or more 3D spherical coils and then filling it with helical coils. Results were evaluated with univariate analysis. Multivariate analysis was used to identify independent predictors of these results.
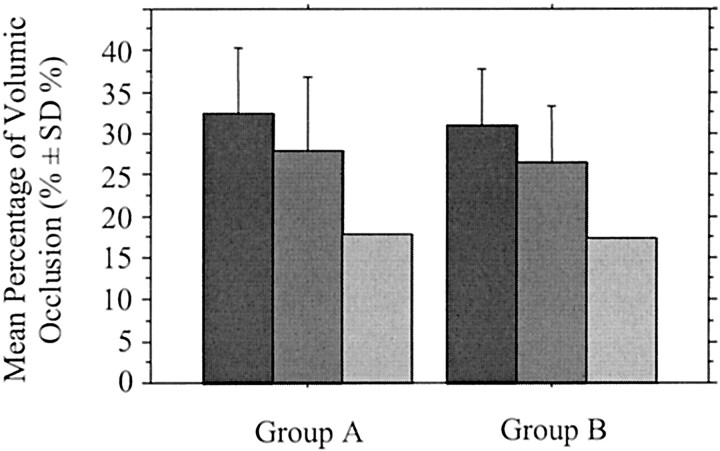
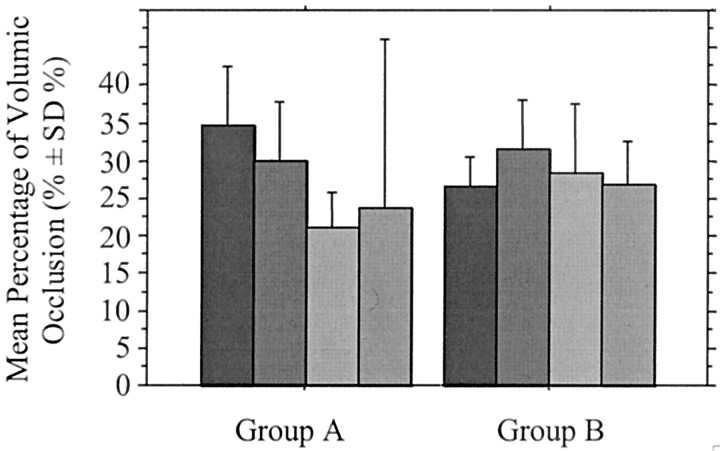
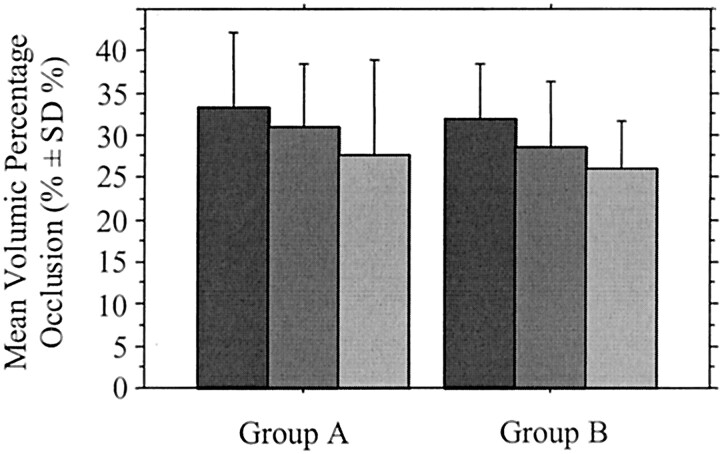
Results: Angiographic occlusion was complete in 84 (72%) and 30 (68%) aneurysms in groups A and B, respectively. Mean percentage of volumic occlusion in these groups was 30.9% and 29.2%, respectively. Perioperative morbidity and mortality rates were 4%, respectively, in group A and 2%, respectively, in group B. No significant difference between the two groups was observed. However, percentage of volumic occlusion correlated with sac-to-neck ratio less than 1.5 (P =.061) and with sac size (P =.002) except when three or more 3D coils per aneurysm were used (P =.222). The better the percentage of volumic occlusion, the better the degree of angiographic occlusion (P =.004). Percentage of volumic occlusion was an independent predictor of angiographic complete occlusion (P =.001). World Federation of Neurological Surgeons subarachnoid hemorrhage scale grade 5 was an independent predictor of perioperative mortality (P =.043).
Conclusion: Three-dimensional coils proved to be useful for improving coil packing and angiographic and volumic occlusion of aneurysms with a neck greater than 4 mm, at the time of treatment, provided the sac-to-neck ratio was 1.5 or greater, and the largest number of 3D coils were first positioned.
Figures
References
-
- Guglielmi G, Viñuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach, II: preliminary clinical experience. J Neurosurg 1991;75:8–14 - PubMed
-
- Horowitz MB, Levy E, Kassam A, Purdy PD. Endovascular therapy for intracranial aneurysms: a historical and present status review. Surg Neurol 2002;57:147–158 - PubMed
-
- Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–482 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical