

Laparoscopic Roux-en-Y gastric bypass for recalcitrant gastroesophageal reflux disease in morbidly obese patients
- PMID: 14974657
- PMCID: PMC3015506
Laparoscopic Roux-en-Y gastric bypass for recalcitrant gastroesophageal reflux disease in morbidly obese patients
Abstract
Background and objectives: Gastroesophageal reflux disease (GERD) is commonly associated with morbid obesity (MO). Antireflux surgery has a higher failure rate in MO and addresses only one of the comorbidities present. This paper reviews the results of laparoscopic Roux-en-Y gastric bypass (LRYGBP) performed for recalcitrant GERD in MO.
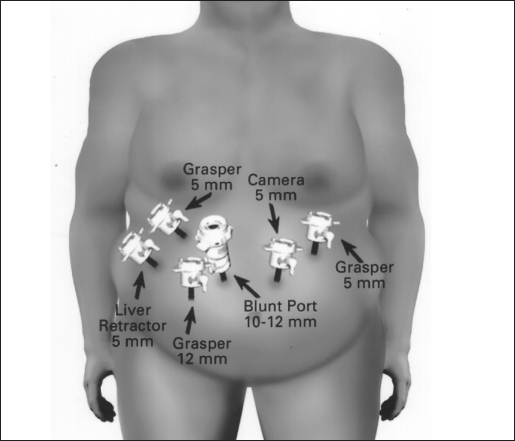
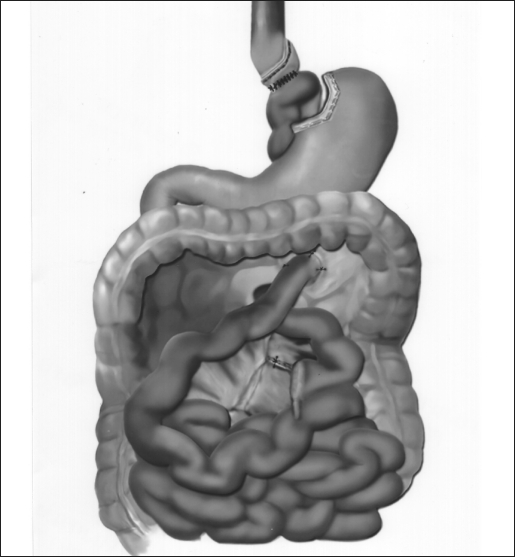
Methods: Patients with recalcitrant GERD and a body mass index (BMI)>35 undergoing LRYGBP were included. LRYGB included crural repair, creation of a small gastric pouch (30 mL), and intestinal bypass (150 to 180 cm). All patients were followed in clinic and by telephone.
Results: From February 1999 to April 2001, 57 patients (51 F, 6 M) with a mean age of 43 (range, 22 to 67) and a median BMI of 43 underwent LRYGBP. Hiatal hernia or esophagitis, or both, were present in 48, Barrett's in 2. LRYGBP was possible in 52 patients; 5 required open conversion. The median hospital stay was 3 days. Complications included 1 leak, 1 pulmonary emboli, 2 reoperations for internal roux limb hernia, and 7 gastrojejunal strictures. At a mean follow-up of 18 months (range, 3 to 30), all patients report improvement or no symptoms of GERD and a mean weight loss of 40 kg (range, 16 to 70). Quality of life scores (SF-36) were above national norms for physical and mental components (median 55, norms=50). GERD-health related quality of life median score was <1 (scale, 0 to 45, 0=asymptomatic, 45=worse).
Conclusion: LRYGBP was effective for recalcitrant GERD in MO. LRYGBP also led to weight loss and improvement in other comorbidites. Surgeons with minimally invasive expertise should consider LRYGBP for treatment of GERD in the morbidly obese.
Figures
References
-
- Duranceau A, Jamieson GG. Hiatal hernia and gastroesophageal reflux. In: Sabiston DCJ, Lyerly HK. eds. Textbook of Surgery. Philadelphia, PA: WB Saunders; 1997: 767– 783
-
- Peters JH, DeMeester TR. Indications, benefits and outcome of laparoscopic Nissen fundoplication. Dig Dis. 1996; 14 ( 3): 169– 179 - PubMed
-
- Trus TL, Laycock WS, Branum G, Waring JP, Mauren S, Hunter JG. Intermediate follow-up of laparoscopic antireflux surgery. Am J Surg. 1996; 171 ( 1): 32– 35 - PubMed
-
- Hinder RA, Raiser F, Katada N, McBride PJ, Perdikis G, Lund RJ. Results of Nissen fundoplication. A cost analysis. Surg Endosc. 1995; 9 ( 12): 1328– 1332 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous