

Sporadic gastric carcinoid tumor laparoscopically resected: a case report
- PMID: 14974672
- PMCID: PMC3015503
Sporadic gastric carcinoid tumor laparoscopically resected: a case report
Abstract
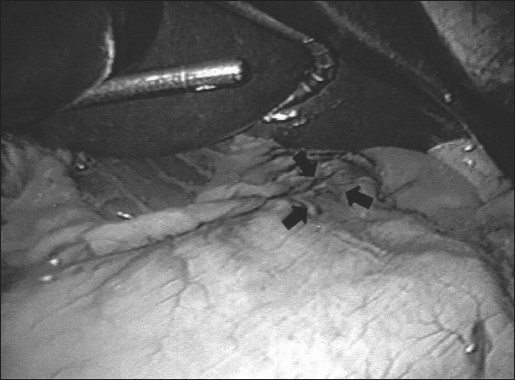
Sporadic gastric carcinoid tumors are relatively infrequent malignancies of the stomach. Tumors measuring less than 1 cm can sometimes be safely removed endoscopically; however, larger neoplasias require surgical ablation. The present case report represents a gastric carcinoid tumor laparoscopically resected in a patient with a history of hematemesis. The tumor was first marked endoscopically with India ink, which facilitated subsequent localization of the area to be resected. Laparoscopic resection of the mass was without complication, and the pathology study confirmed the preoperative diagnosis and negativity of the margins. In patients who present with masses that are not amended for endoscopic resection, sporadic gastric carcinoid tumors can be resected laparoscopically.
Figures



Similar articles
-
A case of sporadic gastric carcinoid tumor treated successfully by laparoscopy-assisted distal gastrectomy.Surg Laparosc Endosc Percutan Tech. 2005 Dec;15(6):348-50. doi: 10.1097/01.sle.0000191588.84485.03. Surg Laparosc Endosc Percutan Tech. 2005. PMID: 16340567
-
Total gastrectomy for type 1 gastric carcinoid: an unusual surgical indication?Minerva Chir. 2007 Oct;62(5):421-4. Minerva Chir. 2007. PMID: 17947953
-
Laparoscopic antrectomy for retained antrum in type 1 gastric carcinoid: a case report and review of literature.Pancreas. 2013 Aug;42(6):1040-2. doi: 10.1097/MPA.0b013e31827e2d3b. Pancreas. 2013. PMID: 23851438 Review. No abstract available.
-
En-bloc resection of multiple type 1 gastric carcinoid tumors by endoscopic multi-band mucosectomy.J Gastroenterol Hepatol. 2009 Sep;24(9):1516-21. doi: 10.1111/j.1440-1746.2009.05909.x. J Gastroenterol Hepatol. 2009. PMID: 19743997
-
A case report of duodenal carcinoid tumor associated with early gastric cancer.J Nippon Med Sch. 2004 Jun;71(3):198-202. doi: 10.1272/jnms.71.198. J Nippon Med Sch. 2004. PMID: 15226611 Review.
References
-
- Akerstrom G. Management of carcinoid tumors of the stomach, duodenum, and pancreas. World J Surg. 1996; 20: 173– 182 - PubMed
-
- Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: a clinicopathologic study. Gastroenterol. 1993; 105 ( 4): 1264– 1266 - PubMed
-
- Tonyonaga T, Nakamura K, Araki Y, Shimura H, Tanaka M. Laparoscopic treatment of duodenal carcinoid tumor. Surg Endosc. 1998; 12: 1085– 1087 - PubMed
-
- Blanc P, Porcheron J, Pages A, Breton C, Mosnier JF, Balique JG. Laparoscopic resection of a duodenal carcinoid tumor. Ann Chir. 2000; 125: 176– 178 - PubMed
-
- Leinati A, Icovoni P, Cavallero G, et al. The carcinoid of Meckel's diverticulum. Minerva Chir. 1995; 50: 501– 504 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical