

Survival after surgery or therapeutic catheterisation for congenital heart disease in children in the United Kingdom: analysis of the central cardiac audit database for 2000-1
- PMID: 14982866
- PMCID: PMC381132
- DOI: 10.1136/bmj.38027.613403.F6
Survival after surgery or therapeutic catheterisation for congenital heart disease in children in the United Kingdom: analysis of the central cardiac audit database for 2000-1
Abstract
Objectives: To analyse simple national statistics and survival data collected in the central cardiac audit database after treatment for congenital heart disease and to provide long term comparative statistics for each contributing centre.
Design: Prospective, longitudinal, observational, national cohort survival study.
Setting: UK central cardiac audit database.
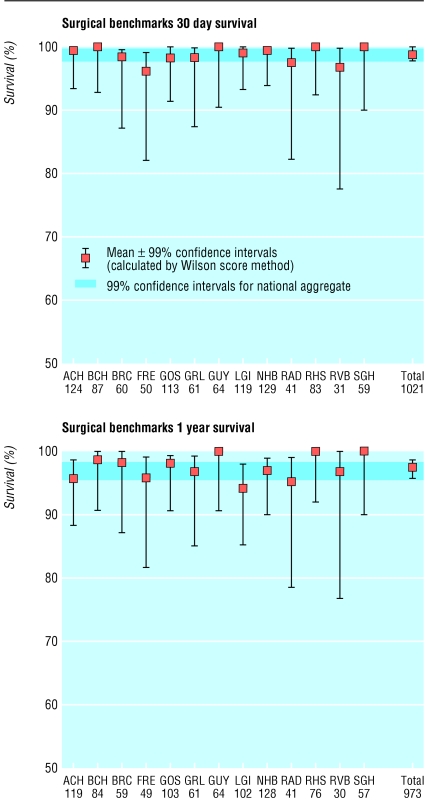
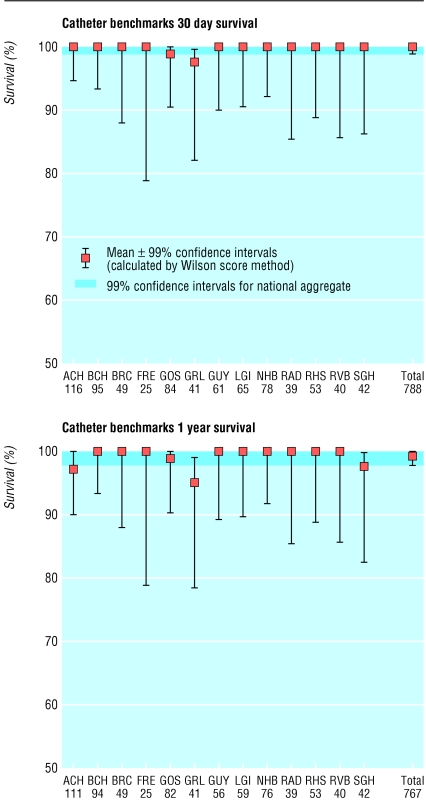
Main outcome measures: Survival at 30 days and one year after treatment in the year April 2000-March 2001, assessed by using both volunteered life status and independently validated life status through the Office for National Statistics, using the patient's unique NHS number, or the general register offices of Scotland and Northern Ireland. Institutional results following a group of six benchmark operations and three benchmark catheterisation procedures.
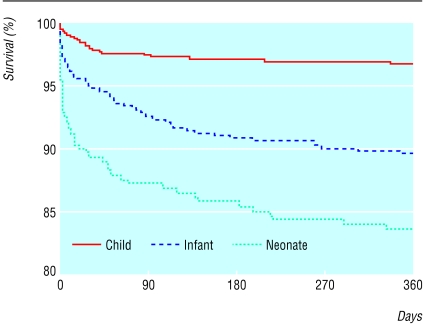
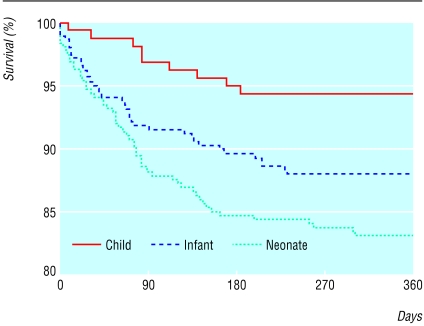
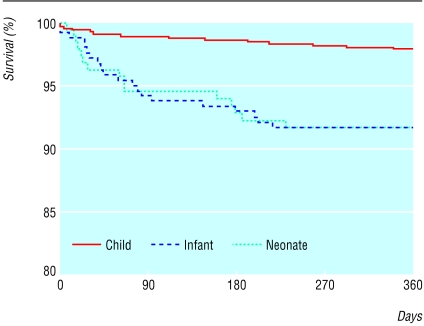
Results: Since April 2000 data have been received from all 13 UK tertiary centres performing cardiac surgery or therapeutic cardiac catheterisation in children with congenital heart disease. Altogether 3666 surgical procedures and 1828 therapeutic catheterisations were performed. Central tracking of mortality identified 469 deaths, 194 occurring within 30 days and 275 later. Forty two of the 194 deaths within 30 days were detected by central tracking but not by volunteered data. For surgery overall, survival at 30 days was 94.9%, falling to 91.2% at one year; this effect was most marked for infants. For therapeutic catheterisation survival at 30 days was 99.1%, falling to 98.1% at one year. Survival of individual centres or individual operators did not differ from the national average after benchmark procedures.
Conclusions: Independent data validation is essential for accurate survival analysis. One year survival gives a more realistic view of outcome than traditional perioperative mortality. Currently no detectable difference exists in survival between any of the 13 UK tertiary congenital heart disease centres, but confidence intervals for small centres are wide, limiting our power to detect underperformance from analysis of a single year's data. Appropriately resourced, focused national audit is capable of accurate data collection on which nationwide, long term quality control can be based.
Figures
Comment in
-
Congenital heart disease.BMJ. 2004 Mar 13;328(7440):594-5. doi: 10.1136/bmj.328.7440.594. BMJ. 2004. PMID: 15016663 Free PMC article. No abstract available.
References
-
- Wilson EB. Probable inference, the law of succession, and statistical inference. J Am Stat Assoc 1927;22: 209-12.
-
- Newcombe R. Two sided confidence intervals for the single proportion: a comparative evaluation of seven methods. Stat Med 1998;17: 857-72. - PubMed
-
- Mavroudis C, Jacobs JP. Congenital heart surgery nomenclature and database project: Overview and minimum dataset. Ann Thorac Surg 2000;69: S2-17. - PubMed
-
- Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, Iezzoni LI. Consensus-based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg 2002;123: 110-18. - PubMed
-
- Gallivan S, Davis KB, Stark JF. Early identification of divergent performance in congenital cardiac surgery. Eur J Cardiothorac Surg 2001;20: 1214-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous