

Experimental model of pediatric asphyxial cardiopulmonary arrest in rats
- PMID: 14987343
- PMCID: PMC3235952
- DOI: 10.1097/01.pcc.0000112376.29903.8f
Experimental model of pediatric asphyxial cardiopulmonary arrest in rats
Abstract
Objective: Develop a clinically relevant model of pediatric asphyxial cardiopulmonary arrest in rats.
Design: Prospective interventional study.
Setting: University research laboratory.
Subjects: Postnatal day 16-18 rats (n = 9/group).
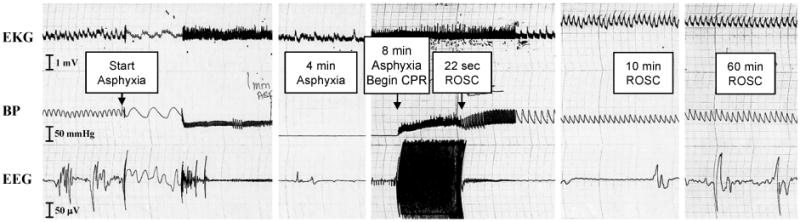
Interventions: Anesthetized rats were endotracheally intubated and mechanically ventilated, and vascular catheters were inserted. Vecuronium was administered, and the ventilator was disconnected from the rats for 8 mins, whereupon rats were resuscitated with epinephrine, sodium bicarbonate, and chest compressions until spontaneous circulation returned. Shams underwent all procedures except asphyxia.
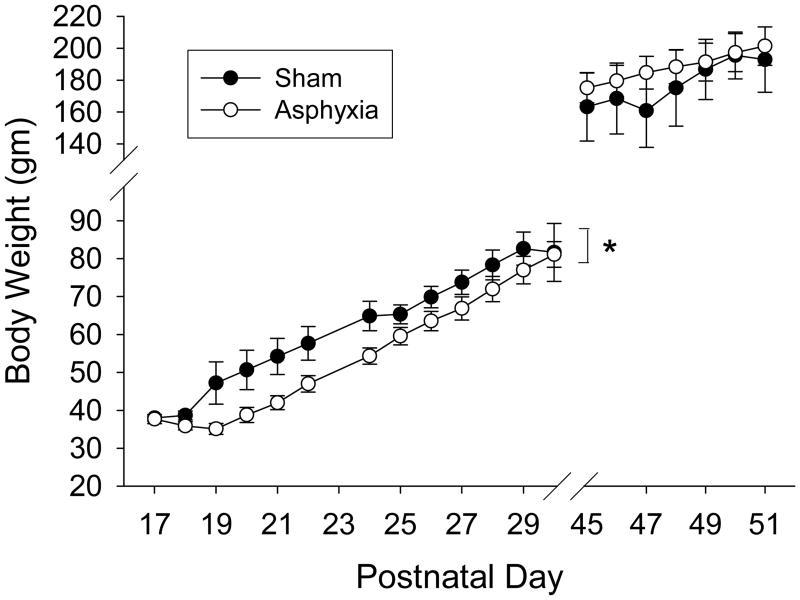
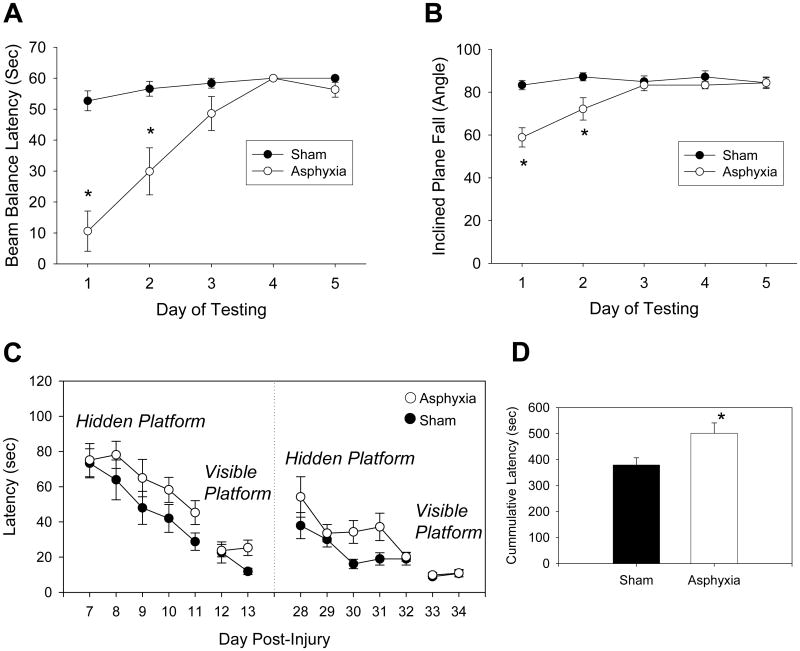
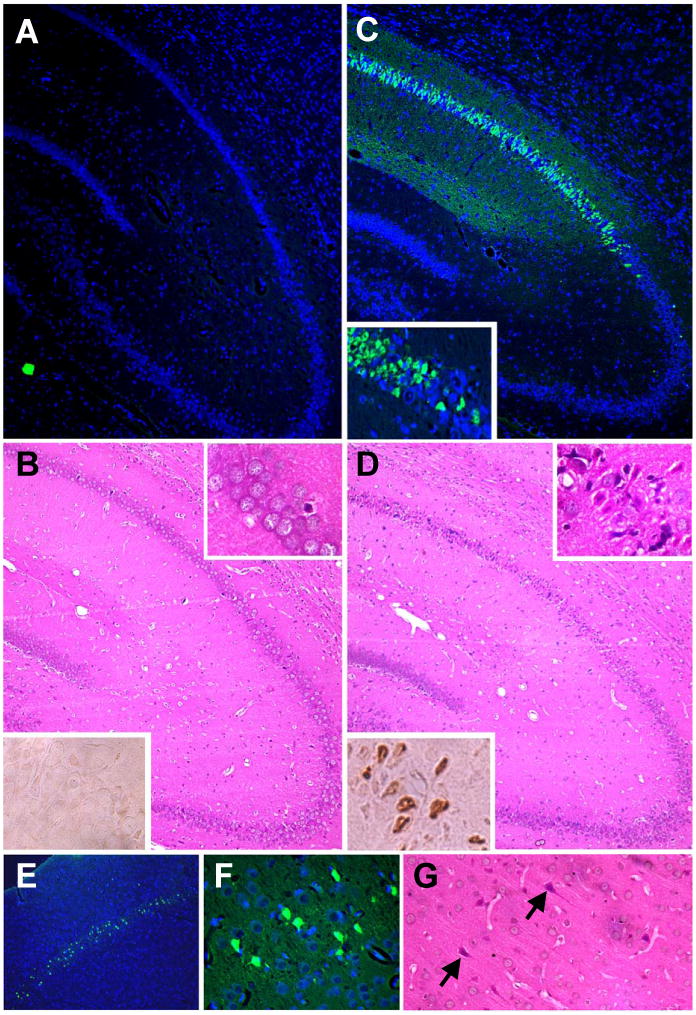
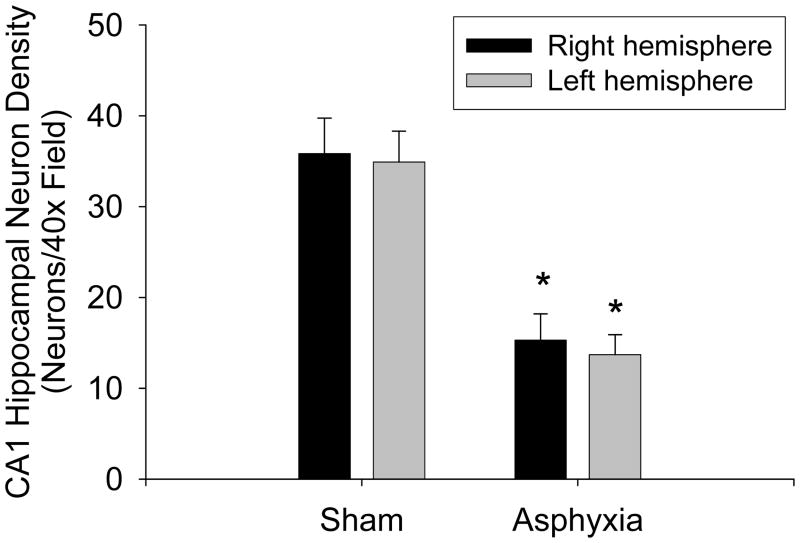
Measurements and main results: Asphyxial arrest typically occurred by 1 min after the ventilator was disconnected. Return of spontaneous circulation typically occurred <30 secs after resuscitation. An isoelectric electroencephalograph was observed for 30 mins after asphyxia, and rats remained comatose for 12-24 hrs. Overall survival rate was 85%. Motor function measured using beam balance and inclined plane tests was impaired on days 1 and 2, but recovered by day 3, in rats after asphyxia vs. sham injury (p <.05). Spatial memory acquisition measured using the Morris-water maze on days 7-14 and 28-35 was also impaired in rats after asphyxia vs. sham injury (total latency 379 +/- 28 vs. 501 +/- 40 secs, respectively, p <.05). DNA fragmentation was detected in CA1 hippocampal neurons bilaterally 3-7 days after asphyxia. Neurodegeneration detected using Fluorojade B was seen in bilateral CA1 hippocampi and layer V cortical neurons 3-7 days after asphyxia, with persistent neurodegeneration in CA1 hippocampus detected up to 5 wks after asphyxia. CA1 hippocampal neuron survival after asphyxia was 39-43% (p <.001 vs. sham). Evidence of DNA or cellular injury was not detected in sham rats.
Conclusions: This model of asphyxial cardiopulmonary arrest in postnatal day 17 rats produces many of the clinical manifestations of pediatric hypoxic-ischemic encephalopathy. This model may be useful for the preclinical testing of novel and currently available interventions aimed at improving neurologic outcome in infants and children after cardiopulmonary arrest.
Figures
References
-
- Young KD, Seidel JS. Pediatric cardiopulmonary resuscitation: a collective review. Ann Emerg Med. 1999;33:195–205. - PubMed
-
- Borta M. Psychosocial issues in water-related injuries. Crit Care Nurs Clin North Am. 1991;3:325–9. - PubMed
-
- Ronco R, King W, Donley DK, et al. Outcome and cost at a children's hospital following resuscitation for out-of-hospital cardiopulmonary arrest. Arch Pediatr Adolesc Med. 1995;149:210–4. - PubMed
-
- Kuisma M, Suominen P, Korpela R. Paediatric out-of-hospital cardiac arrests--epidemiology and outcome. Resuscitation. 1995;30:141–50. - PubMed
-
- Reis AG, Nadkarni V, Perondi MB, et al. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pediatrics. 2002;109:200–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
