

Beneath the calm surface: the changing face of physician-service use in British Columbia, 1985/86 versus 1996/97
- PMID: 14993175
- PMCID: PMC343854
- DOI: 10.1503/cmaj.1020460
Beneath the calm surface: the changing face of physician-service use in British Columbia, 1985/86 versus 1996/97
Abstract
Background: Although expenditures on health care are continually increasing and often said to be unsustainable, few studies have examined these trends at the level of services delivered to individual patients. We analyzed trends in the various components that contributed to changes in overall expenditures for physician services in British Columbia from 1985/86 to 1996/97.
Methods: We obtained data on all fee-for-service payments to physicians in each study year using the British Columbia Linked Health Data set and analyzed these at the level of individual patients. We disaggregated overall billing levels by year into the following components: number of physicians seen by each patient, number of visits per physician, number of services rendered on each visit and average price of those services. We removed the effect of inflation on fees by adjusting to those in 1988. We used direct age-standardization to isolate and measure the effect of demographic changes. We used the Consumer Price Index to determine the effects of inflation.
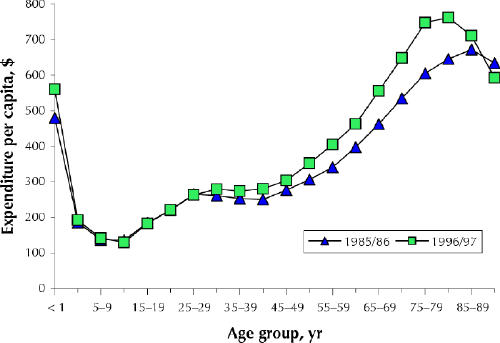
Results: Total payments to fee-for-service physicians in British Columbia rose 86.3% over the study period. The increase was entirely accounted for by the combined effects of population growth (28.9%), aging (2.1%) and general inflation (41.4%). Service use per capita rose 10.5%; this increase was offset by a decline of 9.4% in inflation-adjusted fees. The average cost of age-adjusted per-capita services rendered by general or family practitioners (GP/FPs) increased very little (3.3%) over the 11-year period, compared with a nearly one-third (31.8%) increase for medical specialists. Although there was a dramatic increase in the number of GP/FPs seen on average by each patient (32.9%), this increase was offset by the combination of decreases in the number of visits per physician (-14.9%), the number of services provided per visit (-8.0%) and the "real cost" of each service provided (-3.5%). Visits to medical specialists increased by about 20% over the study period in all age groups. However, for each person 65 years of age or over receiving any services, the average fee-adjusted expenditures increased 24.8%, almost 4 times the rate of increase for people younger than 65. The use of surgical services grew 26.5% for seniors while declining -2.0% for people under age 65.
Interpretation: These findings suggest a form of "homeostasis" in aggregate-level service use and cost. The supposed inflationary effects of population aging and increasing "abuse of the system" by patients were not found.
Figures
Comment in
-
Sustainability of health care in Canada.CMAJ. 2004 May 25;170(11):1646-7; author reply 1647. doi: 10.1503/cmaj.1040426. CMAJ. 2004. PMID: 15159348 Free PMC article. No abstract available.
References
-
- Galbraith JK. The affluent society. Boston: Houghton-Mifflin; 1958.
-
- Barer ML, Evans RG, Hertzman C. Avalanche or glacier? Health care and the demographic rhetoric. Can J Aging 1995;14:193-224.
-
- Evans RG, McGrail KM, Morgan SG, Barer ML, Hertzman C. Apocalypse no: population aging and the future of health care systems. Can J Aging 2001; 20 (Suppl 1):160-91.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous