

Oral contraception does not alter single dose saquinavir pharmacokinetics in women
- PMID: 14998420
- PMCID: PMC1884449
- DOI: 10.1111/j.1365-2125.2003.01983.x
Oral contraception does not alter single dose saquinavir pharmacokinetics in women
Abstract
Aims: Women experience more adverse drug reactions (ADR) to antiretroviral therapy than men. This may be attributed to higher plasma concentrations of protease inhibitors due to pharmacokinetic interactions with hormonal preparations. Thus, in the present study we aimed to investigate the influence of oral contraceptives (OC) on the pharmacokinetics of the protease inhibitor saquinavir.
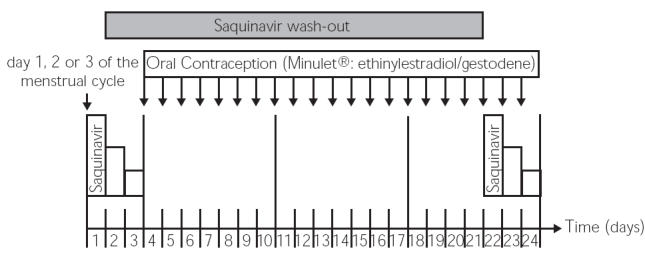
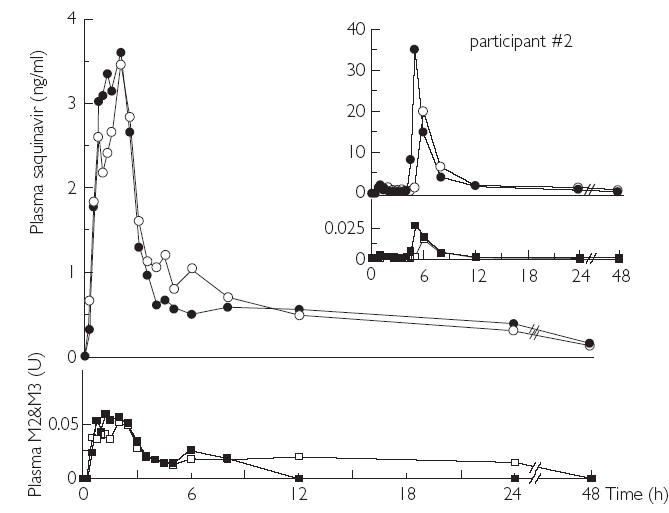
Methods: Saquinavir was administered in a hard gelatin capsule formulation (Invirase) to rule out confounding by pharmaceutical aids of the more frequently used soft gelatin capsule. After an overnight fast, eight healthy female participants ingested a single oral dose of 600 mg saquinavir immediately before and after the 19th dose of a combined, low dose OC (0.03 mg ethinylestradiol, 0.075 mg gestodene) in a prospective, fixed sequence study design. The first saquinavir application was scheduled on day 1, 2, or 3 of the individual menstrual cycle. Plasma concentrations of saquinavir and relative concentrations of its M2&M3-hydroxy metabolites were determined by LC/MS/MS for 48 h.
Results: Intake of OC resulted in a significant decrease in morning serum concentrations (before intake of OC, compared to day 19 of OC therapy) of 17beta-estradiol by -23.4 pg ml-1 (57%, 95%CI: -76% to -37.4%); progesterone by -0.25 ng ml-1 (33%, 95%CI: -45.3% to -21.5%); follicle-stimulating hormone by -4.06 U l-1 (82%, 95%CI: -96.5% to -67.7%); and luteinizing hormone by -3.49 U l-1 (74%, 95%CI: -93 to -54.6%). Conversely, sexual hormone binding globulin serum concentrations increased by 83.6 nmol l-1 (205%, 95%CI: 32.2% to 377%). Pharmacokinetic parameters of saquinavir (AUC, Cmax, tmax, t1/2, CLR) were not affected by OC, nor was the relative metabolic ratio of saquinavir/M2&M3-hydroxy saquinavir. Furthermore, there was no association of serum hormone concentrations or MDR1-polymorphisms (C3435T and G2677T) with pharmacokinetic parameters of saquinavir.
Conclusions: There was no effect of OC on saquinavir pharmacokinetics. Thus, pharmacokinetic interactions of synthetic sexual steroids with saquinavir are not likely to account for the increased ADR to antiretroviral therapy seen in women.
Figures
Similar articles
-
Once-daily dosing of saquinavir and low-dose ritonavir in HIV-1-infected individuals: a pharmacokinetic pilot study.AIDS. 2000 Jun 16;14(9):F103-10. doi: 10.1097/00002030-200006160-00003. AIDS. 2000. PMID: 10894270 Clinical Trial.
-
Pharmacokinetic interactions between sildenafil and saquinavir/ritonavir.Br J Clin Pharmacol. 2000 Aug;50(2):99-107. doi: 10.1046/j.1365-2125.2000.00245.x. Br J Clin Pharmacol. 2000. PMID: 10930961 Free PMC article. Clinical Trial.
-
Lack of sex-related differences in saquinavir pharmacokinetics in an HIV-seronegative cohort.Br J Clin Pharmacol. 2006 Apr;61(4):379-88. doi: 10.1111/j.1365-2125.2006.02593.x. Br J Clin Pharmacol. 2006. PMID: 16542198 Free PMC article.
-
Lopinavir/ritonavir: a review of its use in the management of HIV infection.Drugs. 2003;63(8):769-802. doi: 10.2165/00003495-200363080-00004. Drugs. 2003. PMID: 12662125 Review.
-
Gender: a possible determinant in dosing of dermatologic drugs--an overview.Cutan Ocul Toxicol. 2006;25(3):195-210. doi: 10.1080/15569520600860355. Cutan Ocul Toxicol. 2006. PMID: 16980245 Review.
Cited by
-
U.S. Medical Eligibility Criteria for Contraceptive Use, 2024.MMWR Recomm Rep. 2024 Aug 8;73(4):1-126. doi: 10.15585/mmwr.rr7304a1. MMWR Recomm Rep. 2024. PMID: 39106314 Free PMC article.
-
Impact of Genetic Polymorphisms of ABCB1 (MDR1, P-Glycoprotein) on Drug Disposition and Potential Clinical Implications: Update of the Literature.Clin Pharmacokinet. 2015 Jul;54(7):709-35. doi: 10.1007/s40262-015-0267-1. Clin Pharmacokinet. 2015. PMID: 25860377 Review.
-
Association of the CYP3A5 A6986G (CYP3A5*3) polymorphism with saquinavir pharmacokinetics.Br J Clin Pharmacol. 2004 Oct;58(4):443-4. doi: 10.1111/j.1365-2125.2004.02159.x. Br J Clin Pharmacol. 2004. PMID: 15373940 Free PMC article. No abstract available.
-
Contraception and HIV infection in women.Hum Reprod Update. 2009 Mar-Apr;15(2):165-76. doi: 10.1093/humupd/dmn049. Epub 2008 Nov 1. Hum Reprod Update. 2009. PMID: 18978360 Free PMC article. Review.
-
Contraception in HIV-positive female adolescents.AIDS Res Ther. 2011 Jun 1;8(1):19. doi: 10.1186/1742-6405-8-19. AIDS Res Ther. 2011. PMID: 21631913 Free PMC article.
References
-
- Kando JC, Yonkers KA, Cole JO. Gender as a risk factor for adverse events to medications. Drugs. 1995;50:1–6. - PubMed
-
- Heinemann K, Moehner S, Lewis M, Assmann A, Garbe E, Heinemann LA. Trends of OC use 1980–99 in a German cohort of women. Zentralbl Gynakol. 2002;124:128–31. - PubMed
-
- Wit FW, Weverling GJ, Weel J, Jurriaans S, Lange JM. Incidence of and risk factors for severe hepatotoxicity associated with antiretroviral combination therapy. J Infect Dis. 2002;186:23–31. - PubMed
-
- Lucas GM, Chaisson RE, Moore RD. Highly active antiretroviral therapy in a large urban clinic: risk factors for virologic failure and adverse drug reactions. Ann Intern Med. 1999;131:81–7. - PubMed
-
- Nguyen ML, Nagy GS, Hernandez I, Holtzberg J, Del Rio C, Lennox J. Use of HAART in women: similar response but greater toxicity. XIV. International AIDS Conference; Barcelona. 2002. Abstract WePeB5968.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
