

Senescent impairment in synergistic cytokine pathways that provide rapid cardioprotection in the rat heart
- PMID: 15007092
- PMCID: PMC2212728
- DOI: 10.1084/jem.20031639
Senescent impairment in synergistic cytokine pathways that provide rapid cardioprotection in the rat heart
Abstract
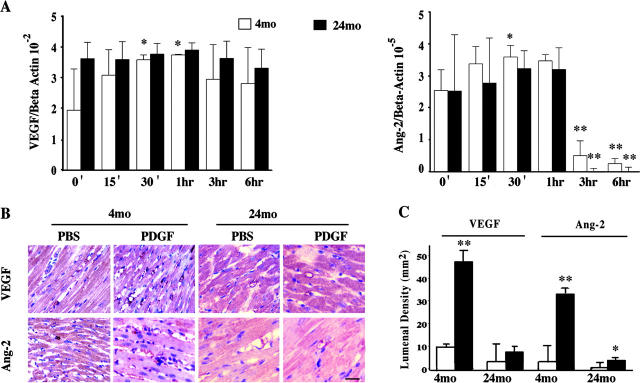
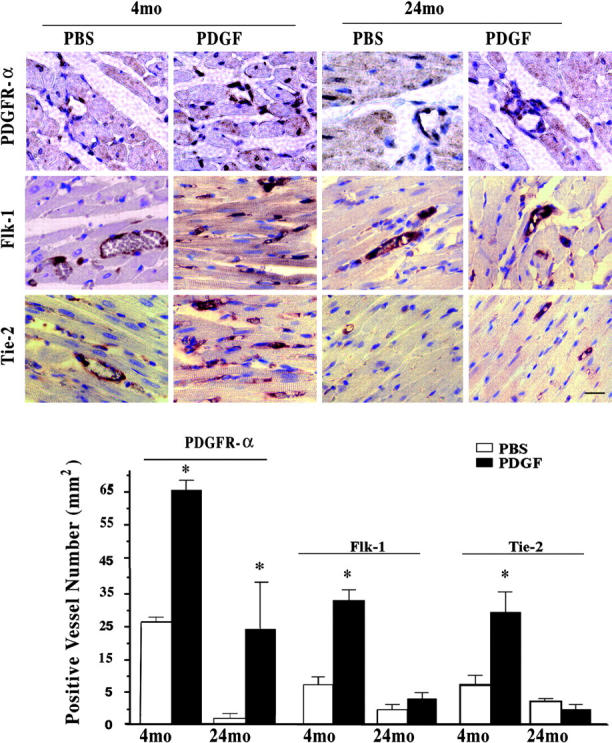
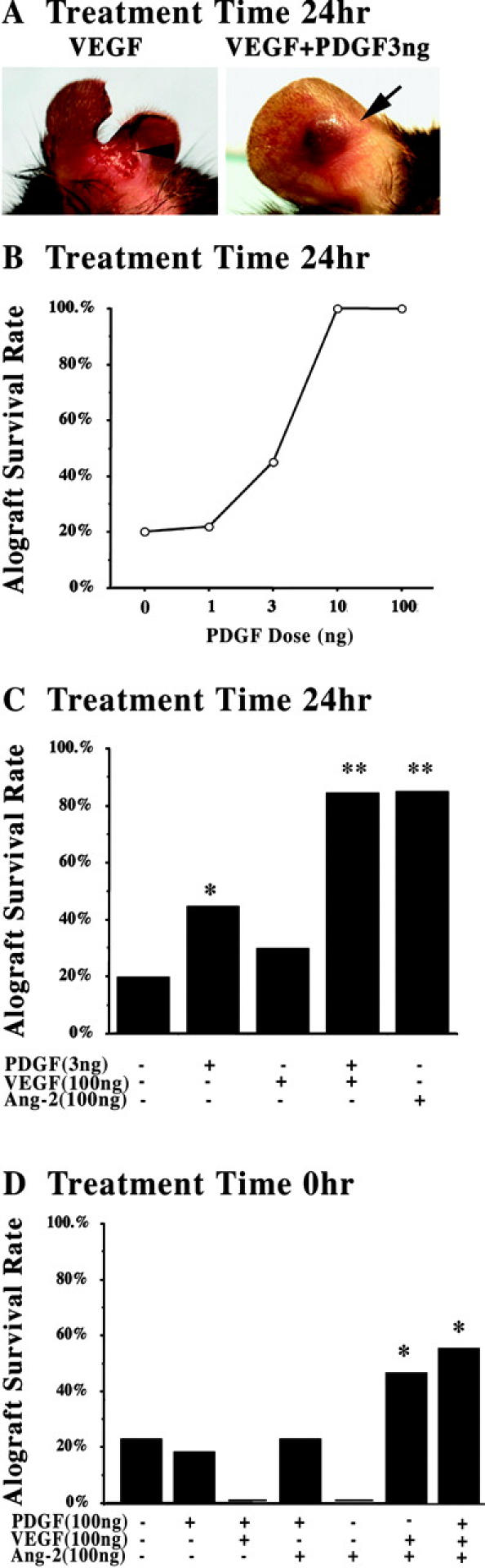
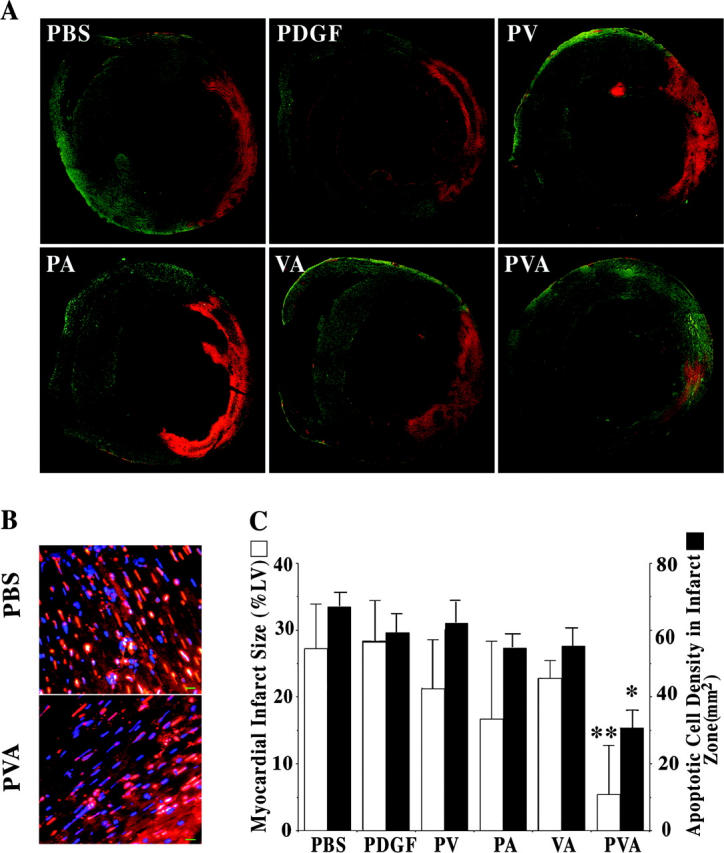
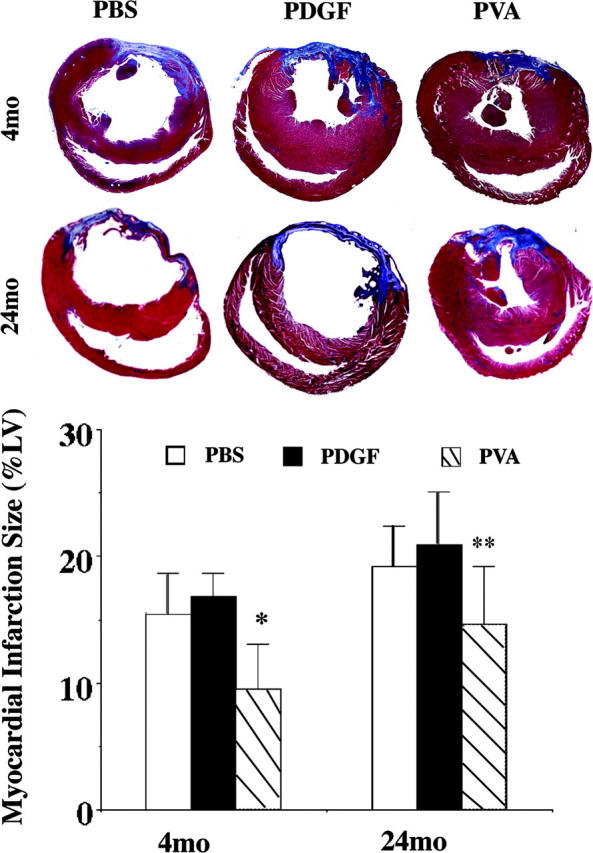
Pretreatment of rodent hearts with platelet-derived growth factor (PDGF)-AB decreases myocardial injury after coronary occlusion. However, PDGF-AB cardioprotection is diminished in older animals, suggesting that downstream elements mediating and/or synergizing the actions of PDGF-AB may be limited in aging cardiac vasculature. In vitro PDGF-AB induced vascular endothelial growth factor (VEGF) and angiopoietin (Ang)-2 expression in 4-mo-old rat cardiac endothelial cells, but not in 24-mo-old heart cells. In vivo injection of young hearts with PDGF-AB increased densities of microvessels staining for VEGF and its receptor, Flk-1, and Ang-2 and its receptor, Tie-2, as well as PDGF receptor (PDGFR)-alpha. In older hearts, PDGF-AB-mediated induction was primarily limited to PDGFR-alpha. Studies in a murine cardiac transplantation model demonstrated that synergist interactions of PDGF-AB plus VEGF plus Ang-2 (PVA) provided an immediate restoration of senescent cardiac vascular function. Moreover, PVA injection in young rat hearts, but not PDGF-AB alone or other cytokine combinations, at the time of coronary occlusion suppressed acute myocardial cell death by >50%. However, PVA also reduced the extent of myocardial infarction with an age-associated cardioprotective benefit (4-mo-old with 45% reduction vs. 24-mo-old with 24%; P < 0.05). These studies showed that synergistic cytokine pathways augmenting the actions of PDGF-AB are limited in older hearts, suggesting that strategies based on these interactions may provide age-dependent clinical cardiovascular benefit.
Figures
References
-
- Kass, D.A. 2002. Age-related changes in venticular-arterial coupling: pathophysiologic implications. Heart Fail. Rev. 7:51–62. - PubMed
-
- Lakatta, E.G., and D. Levy. 2003. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 107:139–146. - PubMed
-
- Halcox, J.P., W.H. Schenke, G. Zalos, R. Mincemoyer, A. Prasad, M.A. Waclawiw, K.R. Nour, and A.A. Quyyumi. 2002. Prognostic value of coronary vascular endothelial dysfunction. Circulation. 106:653–658. - PubMed
-
- Gokce, N., J.F. Keaney, Jr., L.M. Hunter, M.T. Watkins, Z.S. Nedeljkovic, J.O. Menzoian, and J.A. Vita. 2003. Predictive value of noninvasively determined endothelial dysfunction for long-term cardiovascular events in patients with peripheral vascular disease. J. Am. Coll. Cardiol. 41:1769–1775. - PubMed
-
- Edelberg, J.M., S.H. Lee, M. Kaur, L. Tang, N.M. Feirt, S. McCabe, O. Bramwell, S.C. Wong, and M.K. Hong. 2002. Platelet-derived growth factor-AB limits the extent of myocardial infarction in a rat model: feasibility of restoring impaired angiogenic capacity in the aging heart. Circulation. 105:608–613. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
