

Rituximab for chronic recurring thrombotic thrombocytopenic purpura: a case report and review of the literature
- PMID: 15009067
- PMCID: PMC3153075
- DOI: 10.1111/j.1365-2141.2004.04836.x
Rituximab for chronic recurring thrombotic thrombocytopenic purpura: a case report and review of the literature
Abstract
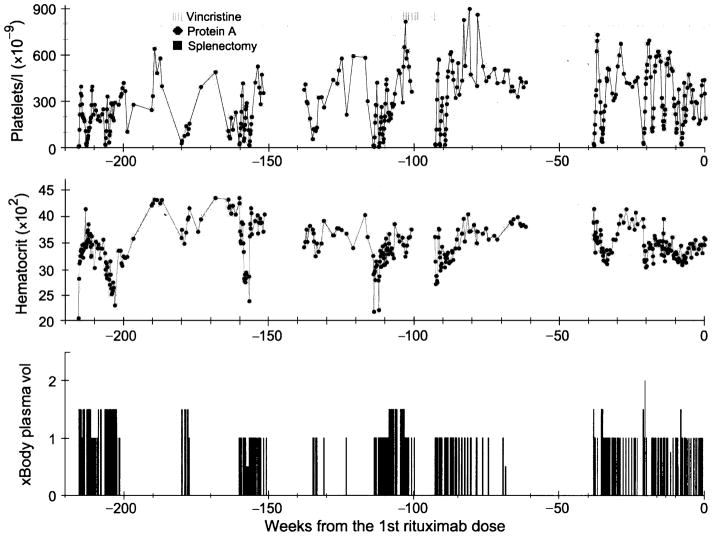
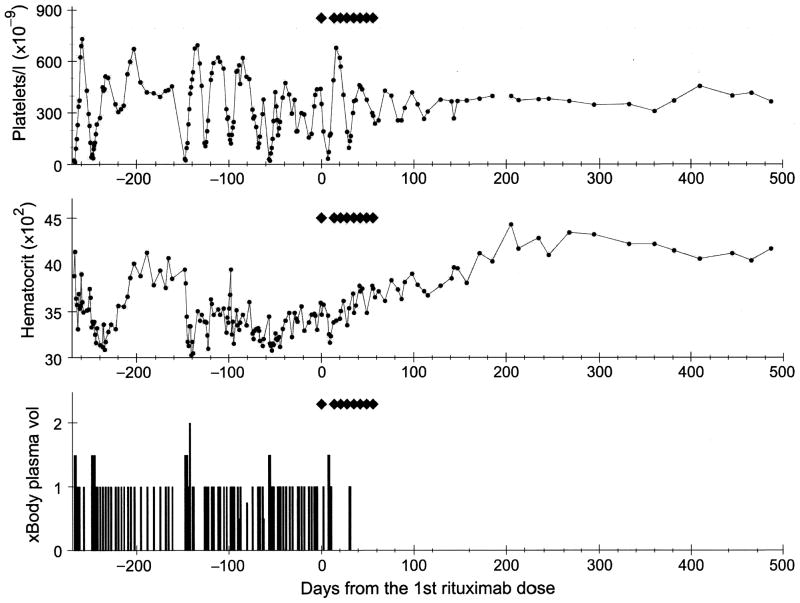
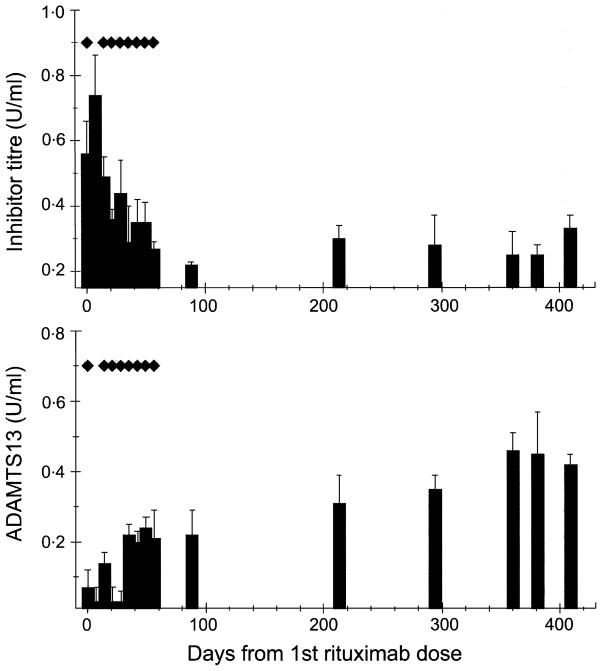
Deficiency of von Willebrand factor (VWF) cleaving protease ADAMTS13 has been demonstrated to be the proximate cause of a subset of thrombotic microangiopathic haemolytic anaemias (MAHA) typical for thrombotic thrombocytopenic purpura (TTP). ADAMTS13 gene mutations cause the hereditary form; acquired deficiency has been attributed to presence of an autoantibody, which may represent a specific subset of MAHA best termed 'autoimmune thrombotic thrombocytopenic purpura'. We describe a patient with relapsing TTP because of ADAMTS13 inhibitors, who failed to achieve sustained remission despite therapies with plasma exchange, steroids, vincristine, staphylococcal protein A and splenectomy. The ADAMTS13 inhibitor titre remained elevated and clinical stability was only maintained by plasma exchange every 2-3 d over a period of 268 d. The patient then received rituximab therapy (eight doses of 375 mg/m2 weekly), during which she required five plasma exchanges in the first 10 d, two exchanges in the next 3 weeks, and none thereafter for 450 d and ongoing. The ADAMTS13 inhibitor titre decreased and enzyme activity increased. We compared this case with that of seven previously reported TTP cases also treated with rituximab; experience suggests that rituximab therapy deserves further investigation for patients with either refractory or relapsing TTP caused by ADAMTS13 inhibitors.
Figures
References
-
- Allford SL, Hunt BJ, Rose P, Machin SJ. Guidelines on the diagnosis and management of the thrombotic microangiopathic haemolytic anaemias. British Journal of Haematology. 2003;120:556–573. - PubMed
-
- Aqui NA, Stein SH, Konkle BA, Abrams CS, Strobl FJ. Role of splenectomy in patients with refractory or relapsed thrombotic thrombocytopenic purpura. Journal of Clinical Apheresis. 2003;18:51–54. - PubMed
-
- Bell WR. Thrombotic thrombocytopenic purpura/hemolytic uremic syndrome relapse: frequency, pathogenesis, and meaning. Seminars in Hematology. 1997;34:134–139. - PubMed
-
- Berentsen S, Tjonnfjord GE, Brudevold R, Gjertsen BT, Langholm R, Lokkevik E, Sorbo JH, Ulvestad E. Favourable response to therapy with the anti-CD20 monoclonal antibody rituximab in primary chronic cold agglutinin disease. British Journal of Haematology. 2001;115:79–83. - PubMed
-
- Boye J, Elter T, Engert A. An overview of the current clinical use of the anti-CD20 monoclonal antibody rituximab. Annals of Oncology. 2003;14:520–535. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
