

The Comorbidity of Major Depression and Anxiety Disorders: Recognition and Management in Primary Care
- PMID: 15014592
- PMCID: PMC181193
- DOI: 10.4088/pcc.v03n0609
The Comorbidity of Major Depression and Anxiety Disorders: Recognition and Management in Primary Care
Abstract
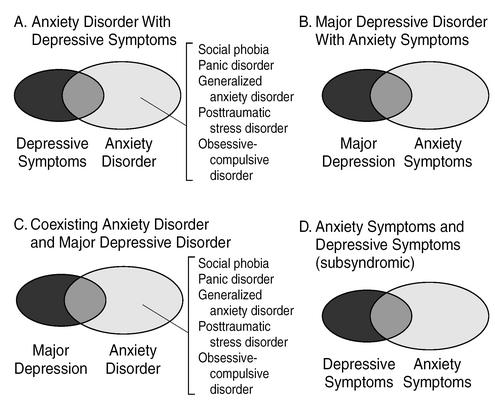
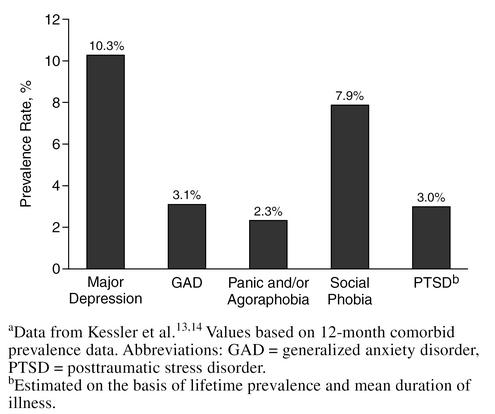
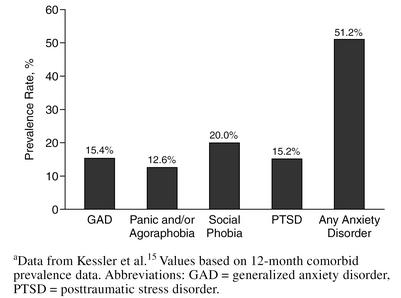
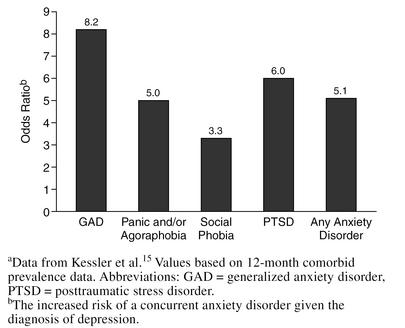
BACKGROUND: Depressive and anxiety disorders commonly occur together in patients presenting in the primary care setting. Although recognition of individual depressive and anxiety disorders has increased substantially in the past decade, recognition of comorbidity still lags. The current report reviews the epidemiology, clinical implications, and management of comorbidity in the primary care setting. METHOD: Literature was reviewed by 2 methods: (1) a MEDLINE search (1980-2001) using the key words depression, depressivedisorders, and anxietydisorders; comorbidity was also searched with individual anxiety diagnoses; and (2) direct search of psychiatry, primary care, and internal medicine journals over the past 5 years. RESULTS: Between 10% and 20% of adults in any given 12-month period will visit their primary care physician during an anxiety or depressive disorder episode (although typically for a nonpsychiatric complaint); more than 50% of these patients suffer from a comorbid second depressive or anxiety disorder. The presence of depressive/anxiety comorbidity substantially increases medical utilization and is associated with greater chronicity, slower recovery, increased rates of recurrence, and greater psychosocial disability. Typically, long-term treatment is indicated, although far less research is available to guide treatment decisions. Selective serotonin reuptake inhibitor antidepressants are the preferred treatment based on efficacy, safety, and tolerability criteria. Knowledge of their differential clinical and pharmacokinetic profiles can assist in optimizing treatment. CONCLUSION: Increased recognition of the high prevalence and negative psychosocial impact of depression and anxiety disorder comorbidity will lead to more effective treatment. While it is hoped that early and effective intervention will yield long-term benefits, research is needed to confirm this.
Figures
References
-
- Murray CJL, Lopez AD. eds. The Global Burden of Disease, vol 1: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Cambridge, Mass: Harvard University Press. 1996
-
- Murray CJL, Lopez AD. eds. The Global Burden of Disease, vol 2: Global Health Statistics. A Compendium of Incidence, Prevalence, and Mortality Estimates for Over 200 Conditions. Cambridge, Mass: Harvard University Press. 1996
-
- Kirmayer LJ, Robbins JM, Dworkind M, et al. Somatization and the recognition of depression and anxiety in primary care. Am J Psychiatry. 1993;150:734–741. - PubMed
-
- Katon W, Von Korff M, Lin E, et al. Distressed high utilizers of medical care: DSM-III-R diagnoses and treatment needs. Gen Hosp Psychiatry. 1990;12:355–362. - PubMed
-
- Schurman RA, Kramer PD, Mitchell JB. The hidden mental health network: treatment of mental illness by nonpsychiatrist physicians. Arch Gen Psychiatry. 1985;42:89–94. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous