

Patient preferences for treatment of rheumatoid arthritis
- PMID: 15020312
- PMCID: PMC1754807
- DOI: 10.1136/ard.2003.019422
Patient preferences for treatment of rheumatoid arthritis
Abstract
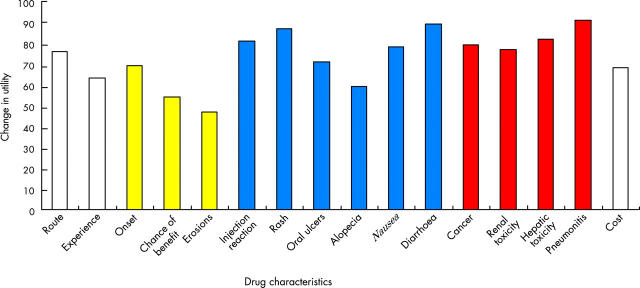
Objective: To elicit treatment preferences of patients with rheumatoid arthritis (RA) for disease modifying antirheumatic drugs (DMARDs) with varying risk profiles.
Methods: Patient values for 16 DMARD characteristics were ascertained using published data about side effects, effectiveness, and cost. Patient preferences were determined by Adaptive Conjoint Analysis, an interactive computer program that predicts preferences by asking patients to make trade-offs between specific treatment characteristics. Simulations were run to derive preferences for four drugs: methotrexate, gold, leflunomide, and etanercept, under different risk-benefit scenarios. Infliximab was not included because it is given with methotrexate, and we did not include preferences for combination therapy. Based on each patient's expressed preferences, and the characteristics of the treatments available at the time of the study, the option that best fitted each patient's perspective was identified.
Results: 120 patients (mean age 70 years) were interviewed. For the base case scenario (which assumed the maximum benefits reported in the literature, a low probability of adverse effects, and low equal monthly "co-pays" (out of pocket costs)), 95% of the respondents preferred etanercept over the other treatment options. When all four options were described as being equally effective, 88% continued to prefer etanercept owing to its safer short term adverse effect profile. Increasing etanercept's co-pay to $30.00 decreased the percentage of patients preferring this option to 80%.
Conclusions: In this study, older patients with RA, when asked to consider trade-offs between specific risk and benefits, preferred etanercept over other treatment options. Preference for etanercept is explained by older patients' risk aversion for drug toxicity.
Figures
Similar articles
-
Comparative effectiveness of tumour necrosis factor alpha inhibitors in combination with either methotrexate or leflunomide.Ann Rheum Dis. 2009 Dec;68(12):1856-62. doi: 10.1136/ard.2008.098467. Epub 2009 Jan 6. Ann Rheum Dis. 2009. PMID: 19126559
-
Etanercept, infliximab, and leflunomide in established rheumatoid arthritis: clinical experience using a structured follow up programme in southern Sweden.Ann Rheum Dis. 2002 Sep;61(9):793-8. doi: 10.1136/ard.61.9.793. Ann Rheum Dis. 2002. PMID: 12176803 Free PMC article.
-
Treatment options for rheumatoid arthritis: celecoxib, leflunomide, etanercept, and infliximab.Ann Pharmacother. 2000 Jun;34(6):743-60. doi: 10.1345/aph.19344. Ann Pharmacother. 2000. PMID: 10860137 Review.
-
Rational use of new and existing disease-modifying agents in rheumatoid arthritis.Ann Intern Med. 2001 Apr 17;134(8):695-706. doi: 10.7326/0003-4819-134-8-200104170-00013. Ann Intern Med. 2001. PMID: 11304108 Review.
-
Safety and efficacy of disease-modifying anti-rheumatic agents: focus on the benefits and risks of etanercept.Drug Saf. 2002;25(3):173-97. doi: 10.2165/00002018-200225030-00004. Drug Saf. 2002. PMID: 11945114 Review.
Cited by
-
Methodologic evaluation of adaptive conjoint analysis to assess patient preferences: an application in oncology.Health Expect. 2010 Dec;13(4):392-405. doi: 10.1111/j.1369-7625.2010.00595.x. Health Expect. 2010. PMID: 20550594 Free PMC article.
-
How Much Information and Participation Do Patients with Inflammatory Rheumatic Diseases Prefer in Interaction with Physicians? Results of a Participatory Research Project.Patient Prefer Adherence. 2019 Dec 17;13:2145-2158. doi: 10.2147/PPA.S209346. eCollection 2019. Patient Prefer Adherence. 2019. PMID: 31908422 Free PMC article.
-
Treatment Mode Preferences in Rheumatoid Arthritis: Moving Toward Shared Decision-Making.Patient Prefer Adherence. 2020 Jan 20;14:119-131. doi: 10.2147/PPA.S220714. eCollection 2020. Patient Prefer Adherence. 2020. PMID: 32021123 Free PMC article.
-
Relative Importance of Disease-Modifying Antirheumatic Drug Attributes for Patients with Rheumatoid Arthritis.Patient Prefer Adherence. 2025 Aug 4;19:2319-2331. doi: 10.2147/PPA.S514920. eCollection 2025. Patient Prefer Adherence. 2025. PMID: 40785840 Free PMC article.
-
Comparison of patient satisfaction with two different etanercept delivery systems. A randomised controlled study in patients with rheumatoid arthritis.Z Rheumatol. 2012 Dec;71(10):890-9. doi: 10.1007/s00393-012-1034-4. Z Rheumatol. 2012. PMID: 22956167 Clinical Trial.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
