

Fellowship training, workload, fatigue and physical stress: a prospective observational study
- PMID: 15023923
- PMCID: PMC359430
- DOI: 10.1503/cmaj.1030442
Fellowship training, workload, fatigue and physical stress: a prospective observational study
Abstract
Background: Fatigue in physician trainees may compromise patient safety and the well-being of the trainees and limit the educational opportunities provided by training programs. Anecdotal evidence suggests that the on-call workload and physical demands experienced by trainees are significant despite duty-hour regulation and support from nursing staff, other trainees and staff physicians.
Methods: We measured the workload and the level of fatigue and physical stress of 11 senior fellows during 35 shifts in the critical care unit at the Hospital for Sick Children in Toronto. We determined number of rostered hours, number of admissions and discharges, number and type of procedures, nurse:patient ratios and related measures of workload. Fellows self-reported the number of pages they received and the amount of time they slept. We estimated physical stress by using a commercially available pedometer to measure the distance walked, by using ambulatory electrocardiographic monitoring to determine arrhythmias and by determining urine specific gravity and ketone levels to estimate hydration.
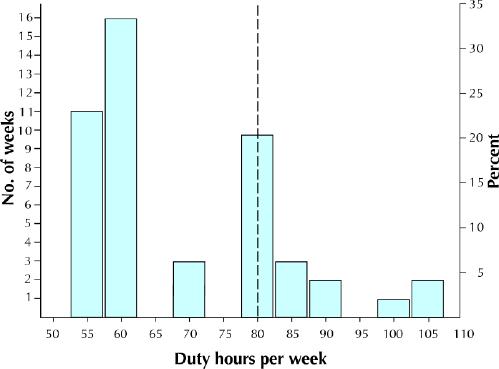
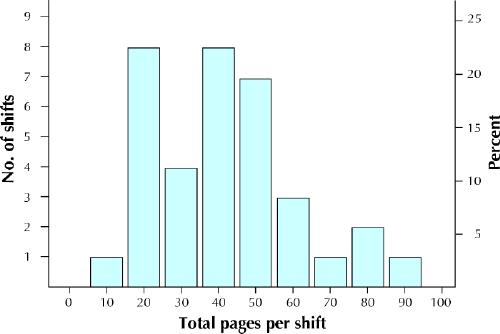
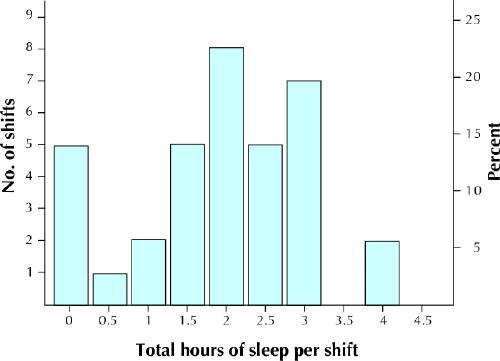
Results: The number of rostered hours were within current Ontario guidelines. The mean shift duration was 25.5 hours (range 24-27 hours). The fellows worked on average 69 hours (range 55-106) per week. On average during a shift, the fellows received 41 pages, were on non-sleeping breaks for 1.2 hours, slept 1.9 hours and walked 6.3 km. Ketonuria was found in participants in 7 (21%) of the 33 shifts during which it was measured. Arrhythmia (1 atrial, 1 ventricular) or heart rate abnormalities occurred in all 6 participants. These fellows were the most senior in-house physician for a mean of 9.4 hours per shift and were responsible for performing invasive procedures in two-thirds of their shifts.
Interpretation: Established Canadian and proposed American guidelines expose trainees to significant on-call workload, physical stress and sleep deprivation.
Figures
Comment in
-
Trainee fatigue: are new limits on work hours enough?CMAJ. 2004 Mar 16;170(6):975-6. doi: 10.1503/cmaj.1031613. CMAJ. 2004. PMID: 15023924 Free PMC article. No abstract available.
-
Preparing physicians for the real world.CMAJ. 2004 Sep 28;171(7):709; author reply 709; discussion 709-10. doi: 10.1503/cmaj.1040528. CMAJ. 2004. PMID: 15451818 Free PMC article. No abstract available.
Similar articles
-
Preparing physicians for the real world.CMAJ. 2004 Sep 28;171(7):709; author reply 709; discussion 709-10. doi: 10.1503/cmaj.1040528. CMAJ. 2004. PMID: 15451818 Free PMC article. No abstract available.
-
Implementing the 2009 Institute of Medicine recommendations on resident physician work hours, supervision, and safety.Nat Sci Sleep. 2011 Jun 24;3:47-85. doi: 10.2147/NSS.S19649. Print 2011. Nat Sci Sleep. 2011. PMID: 23616719 Free PMC article.
-
Evaluating the workload of on-call psychiatry residents: which activities are associated with sleep loss?Acad Psychiatry. 2012 Jan 1;36(1):43-6. doi: 10.1176/appi.ap.10060086. Acad Psychiatry. 2012. PMID: 22362436
-
When policy meets physiology: the challenge of reducing resident work hours.Clin Orthop Relat Res. 2006 Aug;449:116-27. doi: 10.1097/01.blo.0000224057.32367.84. Clin Orthop Relat Res. 2006. PMID: 16770285 Review.
-
Resident duty hours in Canada: a survey and national statement.BMC Med Educ. 2014;14 Suppl 1(Suppl 1):S9. doi: 10.1186/1472-6920-14-S1-S9. Epub 2014 Dec 11. BMC Med Educ. 2014. PMID: 25559388 Free PMC article. Review.
Cited by
-
Less work: more burnout? A comparison of working conditions and the risk of burnout by German physicians before and after the implementation of the EU Working Time Directive.Int Arch Occup Environ Health. 2014 Feb;87(2):205-15. doi: 10.1007/s00420-013-0849-x. Epub 2013 Feb 20. Int Arch Occup Environ Health. 2014. PMID: 23423279
-
Work-Life Balance: The True Failure Is in Not Trying.Front Pediatr. 2016 Apr 28;4:37. doi: 10.3389/fped.2016.00037. eCollection 2016. Front Pediatr. 2016. PMID: 27200320 Free PMC article. Review. No abstract available.
-
The Impact of Sleep and Circadian Disorders on Physician Burnout.Chest. 2019 Nov;156(5):1022-1030. doi: 10.1016/j.chest.2019.07.008. Epub 2019 Jul 25. Chest. 2019. PMID: 31352036 Free PMC article. Review.
-
Stress and Workload Assessment in Aviation-A Narrative Review.Sensors (Basel). 2023 Mar 28;23(7):3556. doi: 10.3390/s23073556. Sensors (Basel). 2023. PMID: 37050616 Free PMC article. Review.
-
Decreased hydration status of emergency department physicians and nurses by the end of their shift.Int J Emerg Med. 2013 Jul 17;6(1):27. doi: 10.1186/1865-1380-6-27. Int J Emerg Med. 2013. PMID: 23866156 Free PMC article.
References
-
- Weinger MB, Ancoli-Israel S. Sleep deprivation and clinical performance. JAMA 2002;287(8):955-7. - PubMed
-
- Gaba DM, Howard SK. Patient safety: fatigue among clinicians and the safety of patients. N Engl J Med 2002;347(16):1249-55. - PubMed
-
- Jha AK, Duncan BW, Bates DW. Fatigue, sleepiness, and medical errors. In: Markowitz AJ, Shojania KG, Duncan BW, McDonald KM, Wachter RM, editors. Making health care safer: a critical analysis of patient safety practices [Evidence Report/Technology Assessment no 43]. San Francisco: Agency for Healthcare Research and Quality; 2003. AHRQ publ. no. 01-E058. Available: www.ahcpr.gov/clinic/ptsafety/ (accessed 2003 Nov 12).
-
- PAIRO–OCOTH agreement. 2000 PAIRO guidelines for trainee practice. Toronto: Professional Association of Internes and Residents of Ontario; 2000.
-
- Philibert I, Friedmann P, Williams WT, ACGME Work Group on Resident Duty Hours, Accreditation Council for Graduate Medical Education. New requirements for resident duty hours. JAMA 2002;288(9):1112-4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous