

High proportion of mutant osteoblasts is compatible with normal skeletal function in mosaic carriers of osteogenesis imperfecta
- PMID: 15024692
- PMCID: PMC1181952
- DOI: 10.1086/383252
High proportion of mutant osteoblasts is compatible with normal skeletal function in mosaic carriers of osteogenesis imperfecta
Abstract
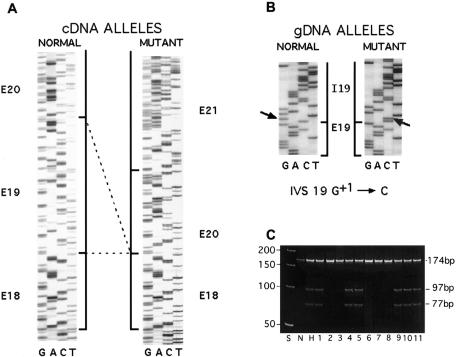
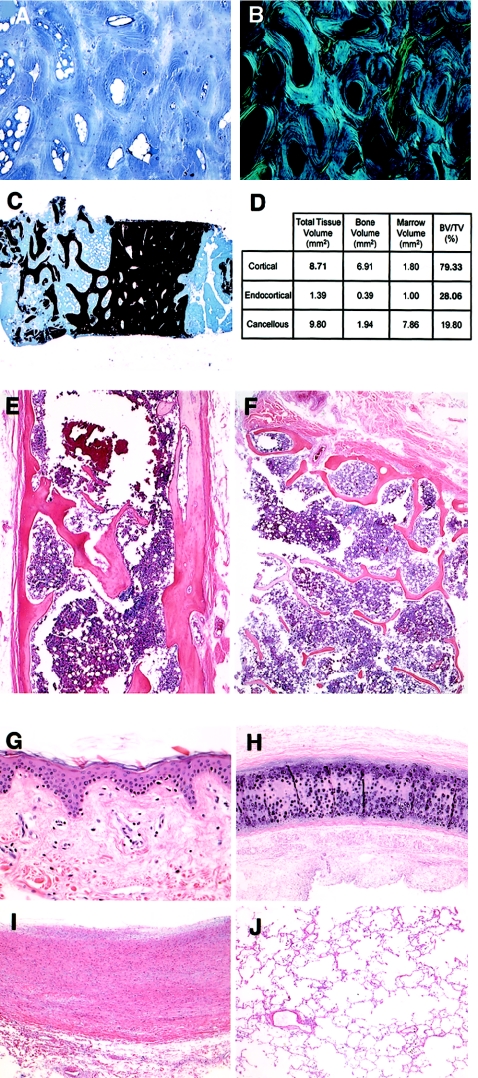
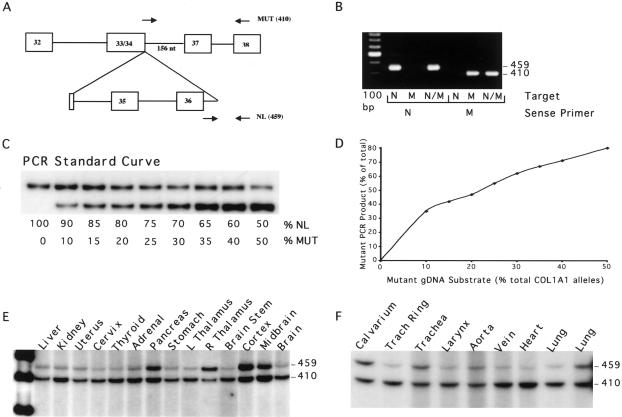
Individuals with mosaicism for the autosomal dominant bone dysplasia osteogenesis imperfecta (OI) are generally identified by having more than one affected child. The mosaic carriers have both normal and mutant cell populations in somatic and germline tissues but are unaffected or minimally affected by the type I collagen mutation that manifests clinically in their heterozygous offspring. We determined the proportion of mutant osteoblasts in skeletal tissue of two mosaic carriers who each have a COL1A1 mutation in a high proportion of dermal fibroblasts. Both carriers had normal height and bone histology; the first carrier had normal lumbar spine measurements (L1-L4), as determined by dual-energy x-ray absorptiometry (Z = +1.17). In cultured cells from the first carrier, studied by labeled PCR and single-cell PCR over successive passages, the collagen mutation was present in 85% of fibroblasts and 50% and 75% of osteoblasts from her right iliac crest and left patella, respectively, with minimal selection. The second carrier was studied by PCR amplification of DNA from autopsy paraffin blocks. The proportion of heterozygous cells was 40% in calvarium, 65% in tracheal ring, and 70% in aorta. Thus, in OI, substantially normal skeletal growth, density, and histology are compatible with a 40%-75% burden of osteoblasts heterozygous for a COL1A1 mutation. These data are encouraging for mesenchymal stem-cell transplantation, since mosaic carriers are a naturally occurring model for cell therapy.
Figures
References
Electronic-Database Information
-
- Database of Type I and III Collagen Mutations, http://www.le.ac.uk/genetics/collagen/
-
- Online Mendelian Inheritance in Man (OMIM), http://www.ncbi.nlm.nih.gov/Omim/ (for OI type I, OI type II, OI type III, and OI type IV)
References
-
- Byers PH, Cole WG (2002) Osteogenesis imperfecta. In: Royce P, Steinmann B (ed) Connective tissue and its heritable disorders, 2nd ed. Wiley-Liss, New York, pp 385–430
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
