

Neurobrucellosis: clinical and neuroimaging correlation
- PMID: 15037461
- PMCID: PMC8158553
Neurobrucellosis: clinical and neuroimaging correlation
Abstract
Background and purpose: Manifestation of nervous system involvement by neurobrucellosis, a treatable infection, is not well documented. We investigated patterns of nervous system involvement and determined if neuroimaging abnormalities correlated with clinical manifestations of neurobrucellosis.
Methods: We reviewed 23 MR imaging studies (17 of brain, six of spine) and seven CT scans of brain in 23 patients (14 male and nine female patients; age range 17-71 years) with positive Brucella titers in their serum and CSF.
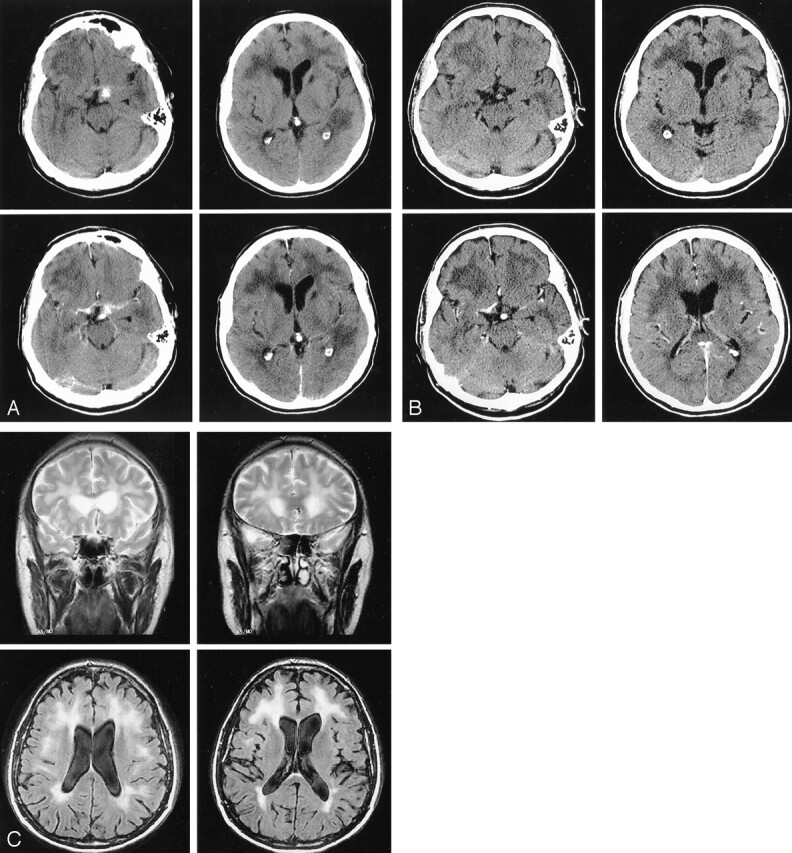
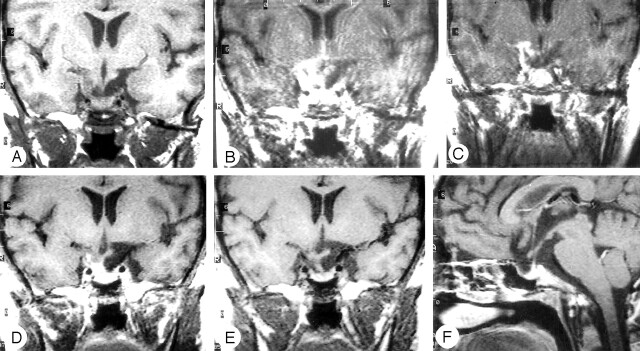
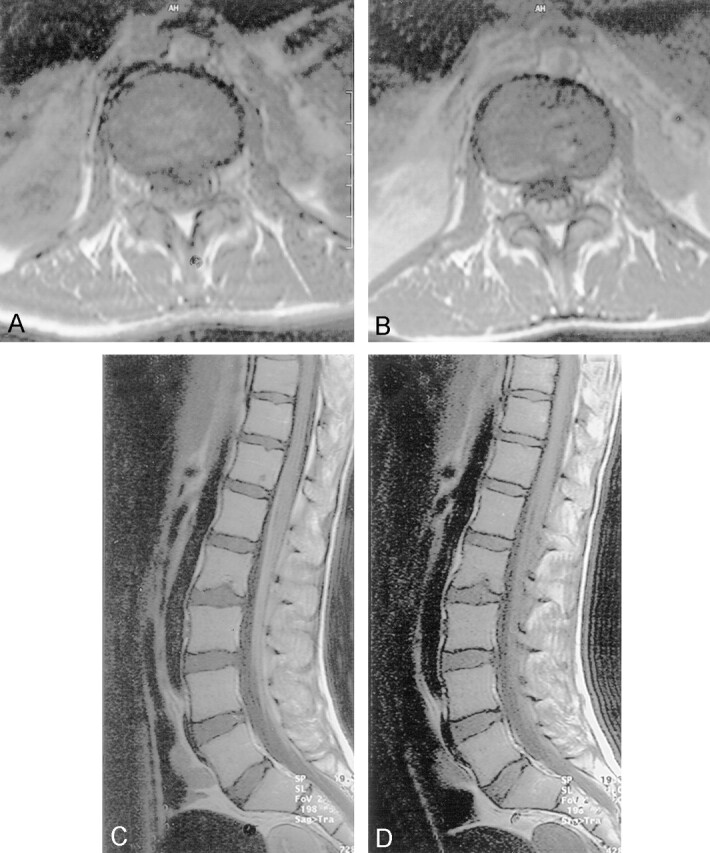
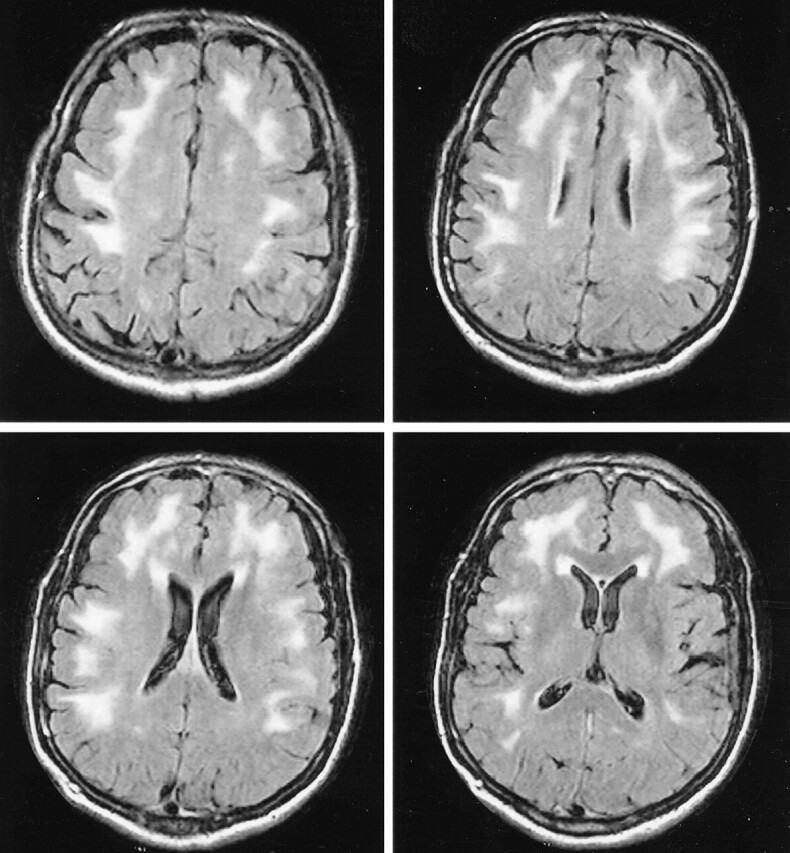
Results: Twelve patients had central nervous system (CNS) involvement, four had peripheral nervous system (PNS) involvement, two had combined PNS and CNS involvement, and five had isolated hearing loss. Imaging findings were variable: five of seven brain CT studies were normal, and 10 of 23 MR studies were normal (eight brain, one thoracic, one lumbar). One brain CT study showed subthalamic hemorrhage, mild perivascular enhancement, left caudate lacunae, and diffuse white matter changes. One other brain CT study showed enhancement of the tentorium in addition to white matter changes. Abnormal MR findings were basal meningeal enhancement (n = 3), lumbar nerve root enhancement (n = 3), granuloma of the suprasellar region (n = 1), diffuse white matter changes (n = 7), and spinal cord atrophy (n = 1). All patients improved after treatment with three antimicrobial drugs for 3-12 months. Seven patients had follow-up imaging; the enhancement disappeared but the white matter and ischemic changes persisted despite almost complete clinical recovery.
Conclusion: Clinical-radiologic correlation in neurobrucellosis varies from a normal imaging study despite positive clinical findings, to a variety of imaging abnormalities that reflect either an inflammatory process, an immune-mediated process, or a vascular insult.
Figures

References
-
- Al- Kawi MZ. Brucellosis. In: Moher JP, Gautier J, eds. Guide to Clinical Neurology, Churchill Livingstone; New York:1995. :677–680
-
- Al Deeb S, Yaqub B, Sharif H, Al-Rajeh SM. Neurobrucellosis. In: Vinken PJ, Bruyn GW, Klawans HL, eds. Hereditary Neuropathies and Spinocerebellar Atrophies, Revised Series 16. Amsterdam: Elsevier Science Publishers;1988. :581–601
-
- Shakir RA. Brucellosis. In: Shakir RA, Neuman PK, Poser CM, eds. Tropical Neurology. Cambridge: WB Saunders;1996. :168–179
-
- Koeck JL, Debord T, Fabre M, Vincent V, Cavallo JD, Le Vagueresse R. Polyradiculopathy with cerebrospinal fluid albuminocytology dissociation due to neurobrucellosis. Clin Infect Dis 1996;23:833–834
MeSH terms
LinkOut - more resources
Full Text Sources
Medical