

Magic angle effects in MR neurography
- PMID: 15037469
- PMCID: PMC8158558
Magic angle effects in MR neurography
Abstract
Background and purpose: Magic angle effects are well recognized in MR imaging of tendons and ligaments, but have received virtually no attention in MR neurography. We investigated the hypothesis that signal intensity from peripheral nerves is increased when the nerve's orientation to the constant magnetic induction field (B(0)) approaches 55 degrees (the magic angle).
Methods: Ten volunteers were examined with their peripheral nerves at different orientations to B(0) to detect any changes in signal intensity and provide data to estimate T2. Two patients with rheumatoid arthritis also had their median nerves examined at 0 degrees and 55 degrees.
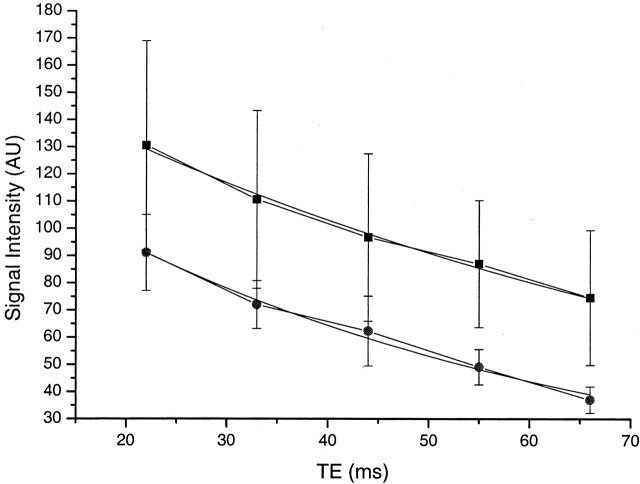
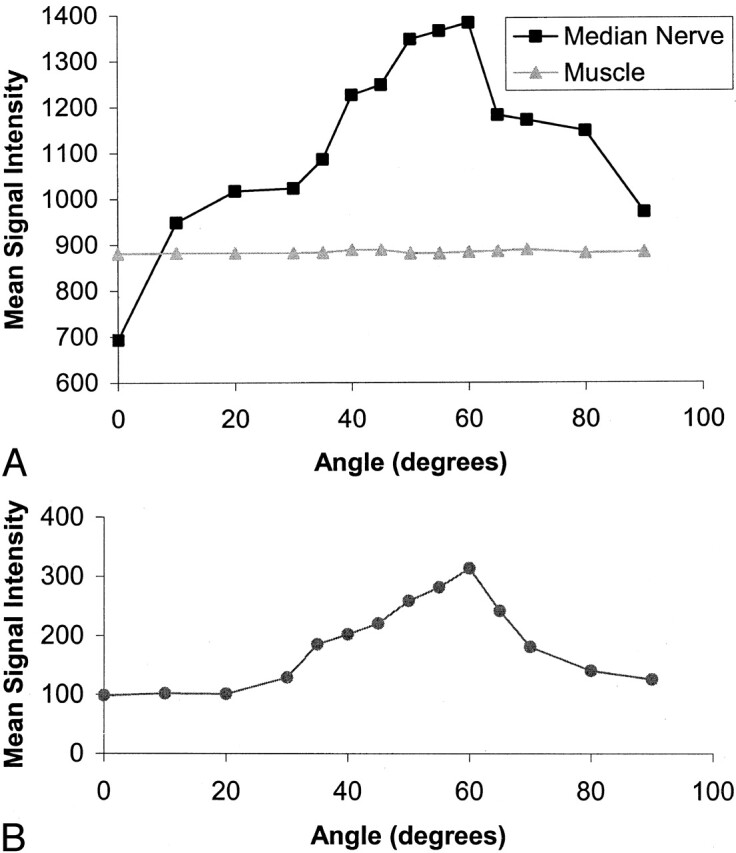
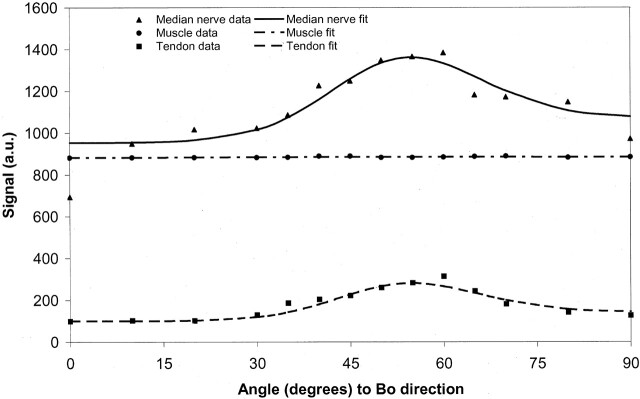
Results: When examined with a short TI inversion-recovery sequence with different TEs, the median nerve showed a 46-175% increase in signal intensity between 0 degrees and 55 degrees and an increase in mean T2 from 47.2 to 65.8 msec. When examined in 5 degrees to 10 degrees increments from 0 degrees to 90 degrees, the median nerve signal intensity changed in a manner consistent with the magic angle effect. No significant change was observed in skeletal muscle. Ulnar and sciatic nerves also showed changes in signal intensity depending on their orientation to B(0). Components of the brachial plexus were orientated at about 55 degrees to B(0) and showed a higher signal intensity than that of nerves in the upper arm that were nearly parallel to B(0). A reduction in the change in signal intensity in the median nerve with orientation was observed in the two patients with rheumatoid arthritis.
Conclusion: Signal intensity of peripheral nerves changes with orientation to B(0). This is probably the result of the magic angle effect from the highly ordered, linearly orientated collagen within them. Differences in signal intensity with orientation may simulate disease and be a source of diagnostic confusion.
Figures







Comment in
-
Peripheral nerve imaging and the magic angle.AJNR Am J Neuroradiol. 2004 Mar;25(3):352-4. AJNR Am J Neuroradiol. 2004. PMID: 15037454 Free PMC article. No abstract available.
References
-
- Aagaard B, Maravilla K, Kliot M. Magnetic resonance neurography: magnetic resonance imaging of the peripheral nerves. Neuroimaging Clin N Am 2001;11:131–146 - PubMed
-
- Blair DN, Rapoport S, Sortman HD, Blair OC. Normal brachial plexus MR imaging. Radiology 1987;165:763–767 - PubMed
-
- Rapoport S, Blair DN, McCarthy SM, Desser TS, Hammes LW, Sortman HD. Brachial plexus: correlation of MR imaging with CT and pathologic findings. Radiology 1987;167:161–165 - PubMed
-
- Posniak HV, Olson MC, Dudiak CM, Wisniewska R, O’Malley C. MR imaging of the brachial plexus. AJR Am J Roentgenol 1993;161:373–379 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical