

Applying a risk-adjustment framework to primary care: can we improve on existing measures?
- PMID: 15043179
- PMCID: PMC1466561
- DOI: 10.1370/afm.6
Applying a risk-adjustment framework to primary care: can we improve on existing measures?
Abstract
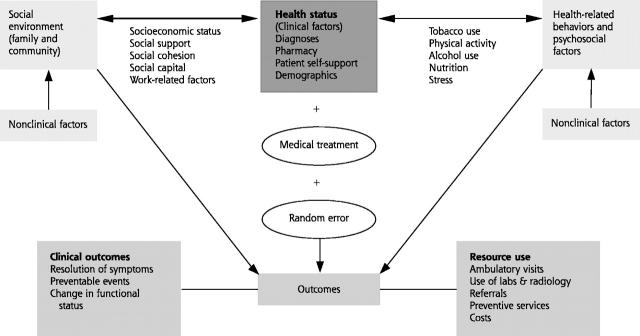
Outcome-based performance measurement and prospective payment are common features of the current managed care environment. Increasingly, primary care clinicians and health care organizations are being asked to assume financial risk for enrolled patients based on negotiated capitation rates. Therefore, the need for methods to account for differences in risk among patients enrolled in primary care organizations has become critical. Although current risk-adjustment measures represent significant advances in the measurement of morbidity in primary care populations, they may not adequately capture all the dimensions of patient risk relevant to primary care. We propose a risk-adjustment framework for primary care that incorporates clinical features related to patients' health status and nonclinical factors related to patients' health behaviors, psychosocial factors, and social environment. Without this broad perspective, clinicians with more unhealthy and more challenging populations are at risk of being inadequately compensated and inequitably compared with peers. The risk-adjustment framework should also be of use to health care organizations that have been mandated to deliver high-quality primary care but are lacking the necessary tools.
Figures
Comment in
-
Chronic illness, comorbidities, and the need for medical generalism.Ann Fam Med. 2003 May-Jun;1(1):4-7. doi: 10.1370/afm.47. Ann Fam Med. 2003. PMID: 15043173 Free PMC article. Review. No abstract available.
References
-
- Fowles J, Weiner JP, Knutson D, Fowler E, Tucker AM. Taking health status into account when setting capitation rates: a comparison of risk adjustment methods. JAMA 1996;276:1316–1321. - PubMed
-
- Hurley J, Hutchison B, Giacomini M, Birch S, Dorland J, Reid R, et al. Policy considerations in implementing capitation for integrated health systems. Ottawa, ON: Canadian Health Services Research Foundation; 1999.
-
- Vanselow NA. Better care and better outcomes: the continuing challenge. JAMA 1998;279:1392–1395. - PubMed
-
- Starfield B. Primary care: balancing health needs, services, and technology. New York, NY: Oxford University Press; 1998.
-
- Institute of Medicine (US). Committee on the Future of Primary Care: America’s Health in a New Era. Washington, DC: National Academy Press; 1996. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources