

Local inhibition of nitric oxide and prostaglandins independently reduces forearm exercise hyperaemia in humans
- PMID: 15047770
- PMCID: PMC1665102
- DOI: 10.1113/jphysiol.2004.061283
Local inhibition of nitric oxide and prostaglandins independently reduces forearm exercise hyperaemia in humans
Abstract
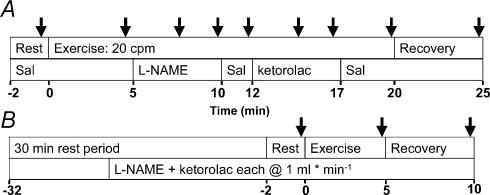
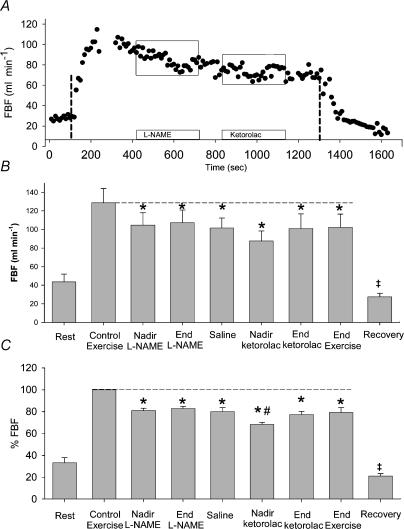
We tested the hypothesis that inhibition of synthesis of either nitric oxide (NO) or vasodilating prostaglandins (PGs) would not alter exercise hyperaemia significantly, but combined inhibition would synergistically reduce the hyperaemia. Fourteen subjects performed 20 min of moderate rhythmic forearm exercise (10% maximal voluntary contraction). Forearm blood flow (FBF) was measured by Doppler ultrasound. Saline or study drugs were infused (2 ml x min(-1)) into the forearm via a brachial artery catheter to locally inhibit synthesis of NO and PGs during steady state exercise (N(G)-nitro-L-arginine methyl ester (L-NAME), 25 mg over 5 min to inhibit NO synthase (NOS); and ketorolac, 3 mg over 5 min to inhibit cyclooxygenase (COX)). After achieving steady state exercise over 5 min (control), L-NAME was infused for 5 min, followed by 2 min saline, then by a 5 min infusion of ketorolac, and finally by 3 min of saline (n= 7). Drug order was reversed in seven additional subjects, such that single inhibition of NOS or COX was followed by combined inhibition. FBF during exercise decreased to 83 +/- 2% of control exercise (100%) with NOS inhibition, followed by a transient decrease to 68 +/- 2% of control during COX inhibition. However, FBF returned to levels similar to those achieved during NOS inhibition within 2 min (80 +/- 3% of control) and remained stable through the final 3 min of exercise. When COX inhibition was performed first, FBF decreased transiently to 88 +/- 4% of control (P < 0.01), and returned to control saline levels by the end of ketorolac infusion. Addition of L-NAME reduced FBF to 83 +/- 3% of control, and it remained stable through to the end of exercise. Regardless of drug order, FBF was approximately 80% of steady state control exercise (P < 0.01) during the last 30 s of exercise. We conclude that (1). NO provides a significant, consistent contribution to hyperaemia, (2). PGs contribute modestly and transiently, suggesting a redundant signal compensates for the loss of vasodilating PGs, and (3). NO and PG signals appear to contribute independently to forearm exercise hyperaemia.
Figures

Comment in
-
Redundancy reflects versatility of blood flow regulation mechanisms.J Physiol. 2004 Jun 1;557(Pt 2):346. doi: 10.1113/jphysiol.2004.066548. Epub 2004 Apr 23. J Physiol. 2004. PMID: 15107476 Free PMC article. No abstract available.
Similar articles
-
Ageing reduces nitric-oxide- and prostaglandin-mediated vasodilatation in exercising humans.J Physiol. 2007 Feb 15;579(Pt 1):227-36. doi: 10.1113/jphysiol.2006.124313. Epub 2006 Nov 30. J Physiol. 2007. PMID: 17138603 Free PMC article. Clinical Trial.
-
Effects of combined inhibition of ATP-sensitive potassium channels, nitric oxide, and prostaglandins on hyperemia during moderate exercise.J Appl Physiol (1985). 2006 May;100(5):1506-12. doi: 10.1152/japplphysiol.01639.2005. Epub 2006 Feb 9. J Appl Physiol (1985). 2006. PMID: 16469932
-
Augmented skeletal muscle hyperaemia during hypoxic exercise in humans is blunted by combined inhibition of nitric oxide and vasodilating prostaglandins.J Physiol. 2011 Jul 15;589(Pt 14):3671-83. doi: 10.1113/jphysiol.2011.209486. Epub 2011 May 30. J Physiol. 2011. PMID: 21624968 Free PMC article.
-
Contribution of non-endothelium-dependent substances to exercise hyperaemia: are they O(2) dependent?J Physiol. 2012 Dec 15;590(24):6307-20. doi: 10.1113/jphysiol.2012.240721. Epub 2012 Oct 8. J Physiol. 2012. PMID: 23045341 Free PMC article. Review.
-
Regulation of blood flow by prostaglandins.Curr Vasc Pharmacol. 2004 Apr;2(2):191-7. doi: 10.2174/1570161043476410. Curr Vasc Pharmacol. 2004. PMID: 15320520 Review.
Cited by
-
Nitric oxide and passive limb movement: a new approach to assess vascular function.J Physiol. 2012 Mar 15;590(6):1413-25. doi: 10.1113/jphysiol.2011.224741. Epub 2012 Feb 6. J Physiol. 2012. PMID: 22310310 Free PMC article. Clinical Trial.
-
Alpha-adrenergic control of blood flow during exercise: effect of sex and menstrual phase.J Appl Physiol (1985). 2010 Nov;109(5):1360-8. doi: 10.1152/japplphysiol.00518.2010. Epub 2010 Aug 19. J Appl Physiol (1985). 2010. PMID: 20724565 Free PMC article. Clinical Trial.
-
Nitric oxide contributes to the augmented vasodilatation during hypoxic exercise.J Physiol. 2010 Jan 15;588(Pt 2):373-85. doi: 10.1113/jphysiol.2009.180489. Epub 2009 Nov 30. J Physiol. 2010. PMID: 19948661 Free PMC article.
-
Tetrahydrobiopterin Administration Augments Exercise-Induced Hyperemia and Endothelial Function in Patients With Systemic Sclerosis.Front Med (Lausanne). 2022 Jan 10;8:791689. doi: 10.3389/fmed.2021.791689. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35083247 Free PMC article.
-
KIR channel activation contributes to onset and steady-state exercise hyperemia in humans.Am J Physiol Heart Circ Physiol. 2014 Sep 1;307(5):H782-91. doi: 10.1152/ajpheart.00212.2014. Epub 2014 Jun 27. Am J Physiol Heart Circ Physiol. 2014. PMID: 24973385 Free PMC article.
References
-
- Bian X, Tune JD, Downey HF. KATP+ channels, nitric oxide, and adenosine are not required for local metabolic coronary vasodilation. Am J Physiol. 2001;281:H831–H837.
-
- Dornyei G, Kaley G, Koller A. Exercise training augments flow-dependent dilation in rat skeletal muscle arterioles. Role of endothelial nitric oxide and prostaglandins. Am J Physiol. 1998;275:H831–H836. - PubMed
-
- Duffy SJ, New G, Tran BT, Harper RW, Meredith IT. Relative contribution of vasodilator prostanoids and no to metabolic vasodilation in the human forearm. Am J Physiol. 1999;276:H663–H670. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous