

Serum LD1 isoenzyme and blood lymphocyte subsets as prognostic indicators for severe acute respiratory syndrome
- PMID: 15049886
- PMCID: PMC7167120
- DOI: 10.1111/j.1365-2796.2004.01323.x
Serum LD1 isoenzyme and blood lymphocyte subsets as prognostic indicators for severe acute respiratory syndrome
Abstract
Background: The pathophysiology of severe acute respiratory syndrome (SARS) is at present poorly understood, but advanced age and serum total lactate dehydrogenase (LD) activity >300 U L(-1) have been associated with adverse clinical outcomes. Blood leucocytes and lymphocyte subsets were reported to decrease, respectively, in 47% and up to 100% of 38 patients in Beijing. However, their prognostic implications have not been thoroughly investigated.
Objective: To investigate serum total LD, LD isoenzymes, and other parameters including blood lymphocyte subsets as prognostic indicators in SARS patients for adverse clinical outcomes in terms of admission to intensive care unit (ICU) and death.
Design: Retrospective analysis.
Subjects and methods: A total of 109 patients with a clinical diagnosis of SARS according to the modified World Health Organization case definition of SARS were recruited from two major acute hospitals in Hong Kong. They were either involved in the initial outbreak of SARS, or cases from the community outbreak of Amoy Gardens between 10 March and 5 May 2003. The clinical diagnosis was subsequently confirmed by serological test and/or molecular analysis. Serum total LD and LD isoenzyme activities, complete blood picture with total leucocyte count and differential counts, absolute counts of CD3+, CD4+, CD8+, natural killer cells and B lymphocytes were measured daily upon admission. Receiver operating characteristic curve analysis was used to determine and compare different cut-offs for various biochemical and immunological parameters at peak serum total LD concentration in predicting adverse clinical outcomes.
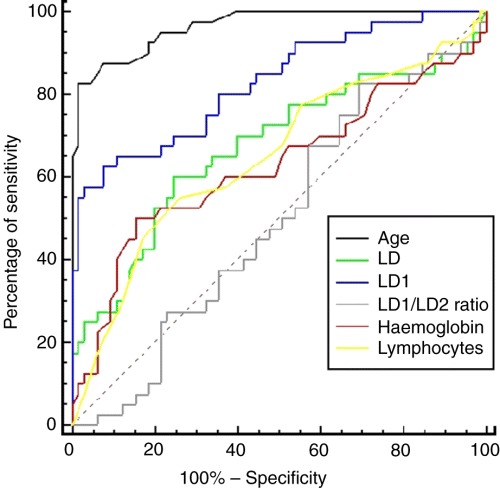
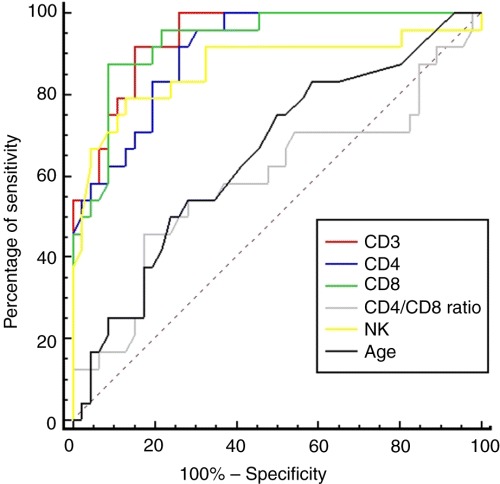
Results: Of a total of 109 patients, 41 were admitted to ICU and 42 died. Of 42 fatal patients, 24 died in ICU and 18 died in general medical wards. Age was found to be an independent prognostic indicator for death with an area under curve (AUC) of 0.96 [95% confidence interval (CI) = 0.90-0.99] but not for admission to ICU [AUC = 0.61 (CI = 0.51-0.70)]. Whilst serum total LD could only achieve AUC of 0.68 (CI = 0.59-0.77) for predicting death, LD1 isoenzyme was found to be the best biochemical prognostic indicator with AUC of 0.84 (CI = 0.75-0.90), sensitivity of 62% (CI = 46-76%), specificity of 93% (CI = 83-98%) at cut-off activity of > or =80 U L(-1). CD3+, CD4+, CD8+ and natural killer cell counts were promising immunological prognostic indicators for predicting admission to ICU with AUC of 0.94 (CI = 0.86-0.98), 0.91 (CI = 0.81-0.96), 0.93 (CI = 0.85-0.98), and 0.87 (CI = 0.76-0.94), respectively.
Conclusions: Apart from age, serum LD1 activity was the best prognostic indicator for predicting death in patients with SARS compared with serum total LD activity, haemoglobin concentration, leucocyte and lymphocyte counts. Its release could possibly be from blood erythrocytes and body tissues other than the myocardium. Blood CD3+, CD4+, CD8+ and natural killer cell counts were found to be good prognostic indicators for predicting admission to ICU in patients with SARS compared with age, leucocyte count and LD isoenzymes. The suppressed CD3+, CD4+, CD8+, and natural killer cell counts were also implicated in the pathophysiology of SARS. Patients with increased serum LD1 should be closely monitored to ensure prompt management, and preparation for admission to ICU could be planned ahead for patients with suppressed lymphocyte subsets.
Conflict of interest statement
We are not aware of any conflicts of interest.
Figures
References
-
- Lee N, Hui D, Wu A et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med 2003; 348: 1986–94. - PubMed
-
- Booth CM, Matukas LM, Tomlinson GA et al. Clinical features and short‐term outcomes of 144 patients with SARS in the Greater Toronto Area. JAMA 2003; 289: 2801–9. - PubMed
-
- Anonymous . Outbreak of severe acute respiratory syndrome ‐ worldwide, 2003. MMWR 2003; 52: 226–8. - PubMed
-
- World Health Organization . Severe acute respiratory syndrome (SARS) – multi‐country outbreak – update 49. http://www.who.int/csr/don/2003_05_07a/en/ (accessed 19 May 2003).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
