

Vasectomy by ligation and excision, with or without fascial interposition: a randomized controlled trial [ISRCTN77781689]
- PMID: 15056388
- PMCID: PMC406425
- DOI: 10.1186/1741-7015-2-6
Vasectomy by ligation and excision, with or without fascial interposition: a randomized controlled trial [ISRCTN77781689]
Abstract
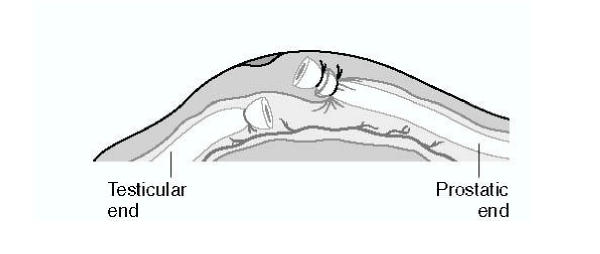
Background: Randomized controlled trials comparing different vasectomy occlusion techniques are lacking. Thus, this multicenter randomized trial was conducted to compare the probability of the success of ligation and excision vasectomy with, versus without, fascial interposition (i.e. placing a layer of the vas sheath between two cut ends of the vas).
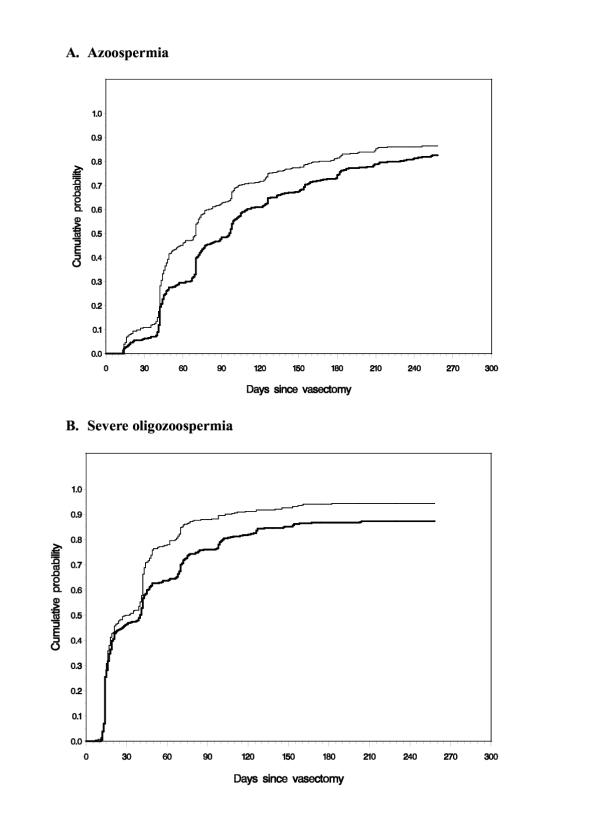
Methods: The trial was conducted between December 1999 and June 2002 with a single planned interim analysis. Men requesting vasectomies at eight outpatient clinics in seven countries in North America, Latin America, and Asia were included in the study. The men were randomized to receive vasectomy with versus without fascial interposition. All surgeons performed the vasectomies using the no-scalpel approach to the vas. Participants had a semen analysis two weeks after vasectomy and then every four weeks up to 34 weeks. The primary outcome measure was time to azoospermia. Additional outcome measures were time to severe oligozoospermia (<100 000 sperm/mL) and vasectomy failure based on semen analyses.
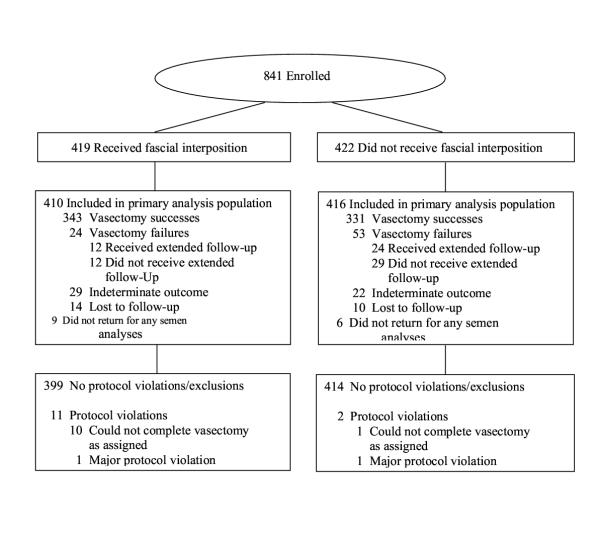
Results: We halted recruitment after the planned interim analysis, when 841 men had been enrolled. Fascial interposition decreased time to azoospermia (hazard ratio [HR], 1.35; P < 0.0001) and time to severe oligozoospermia (HR, 1.32; P < 0.0001) and reduced failures based on semen analysis by about half, from 12.7% (95% confidence interval [CI], 9.7 to 16.3) to 5.9% (95% CI, 3.8 to 8.6) (P < 0.0001). Older men benefited less from fascial interposition than younger men in terms of the speed of achieving azoospermia. However, the number of vasectomy failures was reduced to a similar degree in all age groups. Slightly more adverse events occurred in the fascial interposition group, but the difference was not significant. These failure rates may appear high to practitioners in countries such as the USA, but they are similar to results from other careful studies of ligation and excision techniques.
Conclusion: Fascial interposition significantly improves vasectomy success when ligation and excision is the method of vas occlusion. A limitation of this study is that the correlation between postvasectomy sperm concentrations and risk of pregnancy is not well quantified.
Figures
References
-
- Liskin L, Pile JM, Quillin WF. Population Reports: Male Sterilization Series D. Vol. 4. Baltimore: John Hopkins University, Population Information Program; 1983.
-
- Trussell J, Kowal D. The essentials of contraception. In: Hatcher RA, Trussel J, Stewart F, Cates W, Stewart GK, Guest F, Kowal D, editor. In Contraceptive Technology. 17. New York: Ardent Media; 1998. pp. 211–247.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
